

A real-life experience with eculizumab and efgartigimod in generalized myasthenia gravis patients
- PMID: 39080054
- PMCID: PMC11377599
- DOI: 10.1007/s00415-024-12588-7
A real-life experience with eculizumab and efgartigimod in generalized myasthenia gravis patients
Erratum in
-
Correction: A real-life experience with eculizumab and efgartigimod in generalized myasthenia gravis patients.J Neurol. 2025 Apr 29;272(5):366. doi: 10.1007/s00415-025-13061-9. J Neurol. 2025. PMID: 40299078 Free PMC article. No abstract available.
Abstract
Introduction: Eculizumab, a complement active antibody, and efgartigimod, an Fc fragment that blocks neonatal Fc receptor, are both approved to treat generalized myasthenia gravis (gMG) patients. The objective of this study is to describe the clinical response to both treatments in a real-life setting.
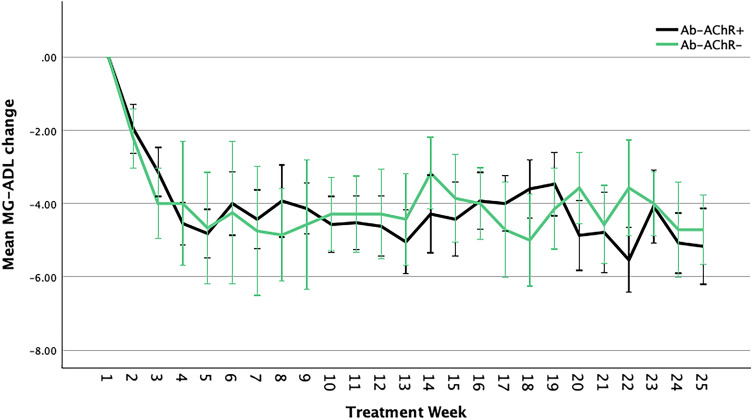
Methods: We collected baseline and follow-up clinical data using the Myasthenia Gravis-Activities of Daily Living (MG-ADL), and Quantitative Myasthenia Gravis (QMG). We included 63 patients, 32 treated with eculizumab and 31 with efgartigimod. Of the efgartigimod-treated patients, 22 were anti-acetylcholine receptor antibody-positive (AChR-Ab +) and 9 were AChR-Ab- (3 MuSK-Ab + and 6 seronegative).
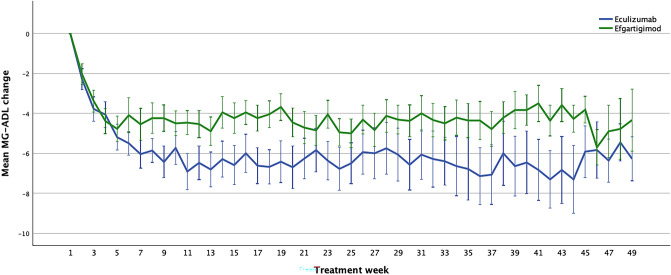
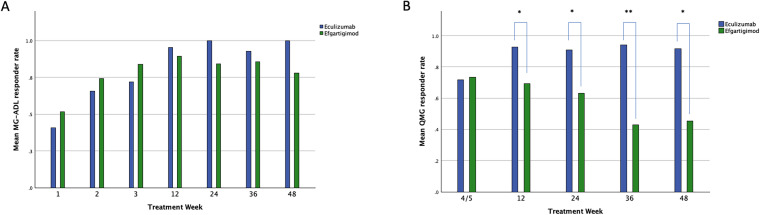
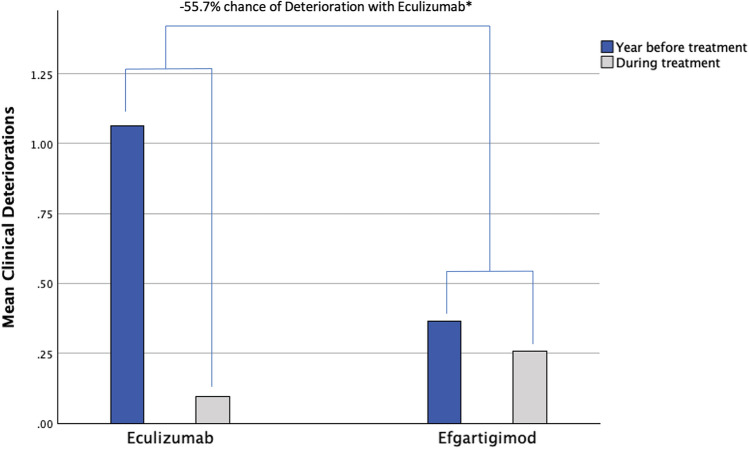
Results: Both treatments showed similar efficacy relative to the MG-ADL scale reduction (p = 0.237). Efgartigimod had a similar effect on both AChR-Ab + and AChR-Ab- (p = 0.280). Eculizumab was superior to efgartigimod relative to the QMG score reduction for the entire dataset (p = 0.003) and was more likely to achieve a clinical response at the QMG compared to efgartigimod (OR 1.373; p = 0.016). Steroid-sparing effect was higher for eculizumab than efgartigimod ( - 16.7 vs - 5.2 mg of the baseline daily dose at follow-up; p = 0.001). Mean speed of prednisone reduction was - 13.1 mg of the daily dose for each month of follow-up for eculizumab-treated patients and - 3.2 for efgartigimod (p = 0.001). We found three serious events, all not related to treatment in the investigator's opinion. One eculizumab-treated patient experienced a severe pneumonia and died despite treatment.
Conclusions: Our study provides evidence that eculizumab and efgartigimod can be used in clinical practice to reduce disability in gMG patients. Eculizumab-treated patients had a higher QMG response and steroid sparing effect. Efgartigimod may offer a more flexible schedule due to its cyclical use, no need for vaccination, and efficacy in AChR-Ab- patients.
Keywords: Innovative; MG-ADL; Observational; QMG; Real-world evidence; Seronegative.
© 2024. The Author(s).
Conflict of interest statement
None.
Figures


References
-
- Howard JF Jr, Utsugisawa K, Benatar M et al (2017) Safety and efficacy of eculizumab in anti-acetylcholine receptor antibody-positive refractory generalised myasthenia gravis (REGAIN): a phase 3, randomised, double-blind, placebo-controlled, multicentre study. Lancet Neurol 16:976–986 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
