

Mechanical power ratio threshold for ventilator-induced lung injury
- PMID: 39080225
- PMCID: PMC11289208
- DOI: 10.1186/s40635-024-00649-0
Mechanical power ratio threshold for ventilator-induced lung injury
Erratum in
-
Correction: Mechanical power ratio threshold for ventilator-induced lung injury.Intensive Care Med Exp. 2024 Sep 12;12(1):79. doi: 10.1186/s40635-024-00666-z. Intensive Care Med Exp. 2024. PMID: 39264545 Free PMC article. No abstract available.
Abstract
Rationale: Mechanical power (MP) is a summary variable incorporating all causes of ventilator-induced-lung-injury (VILI). We expressed MP as the ratio between observed and normal expected values (MPratio).
Objective: To define a threshold value of MPratio leading to the development of VILI.
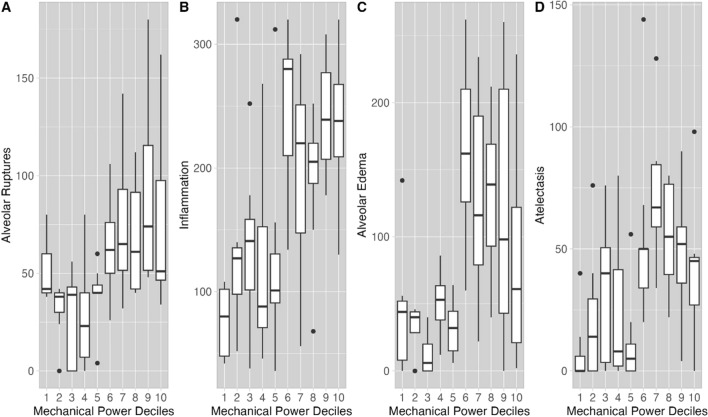
Methods: In a population of 82 healthy pigs, a threshold of MPratio for VILI, as assessed by histological variables and confirmed by using unsupervised cluster analysis was 4.5. The population was divided into two groups with MPratio above or below the threshold.
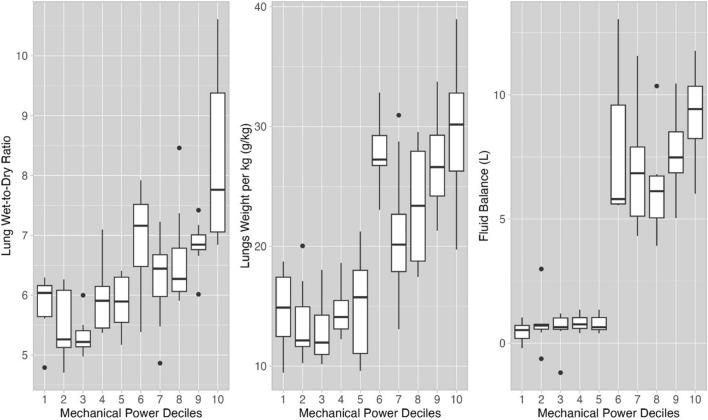
Measurements and main results: We measured physiological variables every six hours. At the end of the experiment, we measured lung weight and wet-to-dry ratio to quantify edema. Histological samples were analyzed for alveolar ruptures, inflammation, alveolar edema, atelectasis. An MPratio threshold of 4.5 was associated with worse injury, lung weight, wet-to-dry ratio and fluid balance (all p < 0.001). After 48 h, in the two MPratio clusters (above or below 4.5), respiratory system elastance, mean pulmonary artery pressure and physiological dead space differed by 32%, 36% and 22%, respectively (all p < 0.001), being worse in the high MPratio group. Also, the changes in driving pressure, lung elastance, pulmonary artery occlusion pressure, central venous pressure differed by 17%, 64%, 8%, 25%, respectively (all p < 0.001).
Limitations: The main limitation of this study is its retrospective design. In addition, the computation for the expected MP in pigs is based on arbitrary criteria. Different values of expected MP may change the absolute value of MP ratio but will not change the concept of the existence of an injury threshold.
Conclusions: The concept of MPratio is a physiological and intuitive way to quantify the risk of ventilator-induced lung injury. Our results suggest that a mechanical power ratio > 4.5 MPratio in healthy lungs subjected to 48 h of mechanical ventilation appears to be a threshold for the development of ventilator-induced lung injury, as indicated by the convergence of histological, physiological, and anatomical alterations. In humans and in lungs that are already injured, this threshold is likely to be different.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
LinkOut - more resources
Full Text Sources
