

Computer-aided prognosis of tuberculous meningitis combining imaging and non-imaging data
- PMID: 39080381
- PMCID: PMC11289120
- DOI: 10.1038/s41598-024-68308-8
Computer-aided prognosis of tuberculous meningitis combining imaging and non-imaging data
Abstract
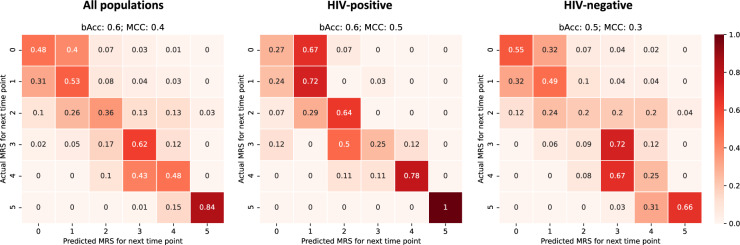
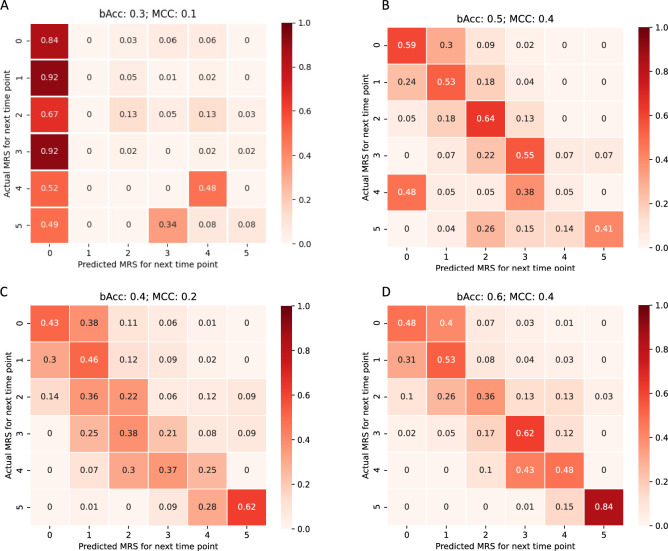
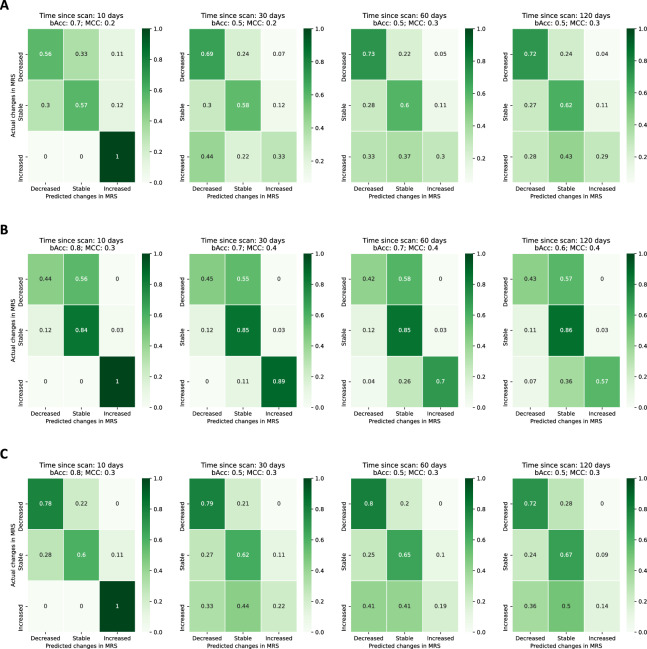
Tuberculous meningitis (TBM) is the most lethal form of tuberculosis. Clinical features, such as coma, can predict death, but they are insufficient for the accurate prognosis of other outcomes, especially when impacted by co-morbidities such as HIV infection. Brain magnetic resonance imaging (MRI) characterises the extent and severity of disease and may enable more accurate prediction of complications and poor outcomes. We analysed clinical and brain MRI data from a prospective longitudinal study of 216 adults with TBM; 73 (34%) were HIV-positive, a factor highly correlated with mortality. We implemented an end-to-end framework to model clinical and imaging features to predict disease progression. Our model used state-of-the-art machine learning models for automatic imaging feature encoding, and time-series models for forecasting, to predict TBM progression. The proposed approach is designed to be robust to missing data via a novel tailored model optimisation framework. Our model achieved a 60% balanced accuracy in predicting the prognosis of TBM patients over the six different classes. HIV status did not alter the performance of the models. Furthermore, our approach identified brain morphological lesions caused by TBM in both HIV and non-HIV-infected, associating lesions to the disease staging with an overall accuracy of 96%. These results suggest that the lesions caused by TBM are analogous in both populations, regardless of the severity of the disease. Lastly, our models correctly identified changes in disease symptomatology and severity in 80% of the cases. Our approach is the first attempt at predicting the prognosis of TBM by combining imaging and clinical data, via a machine learning model. The approach has the potential to accurately predict disease progression and enable timely clinical intervention.
Keywords: DenseNet; Long short-term memory network; MRI imaging; Machine learning; Prognosis; Tuberculous meningitis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
