

Nephrectomy and high-salt diet inducing pulmonary hypertension and kidney damage by increasing Ang II concentration in rats
- PMID: 39080603
- PMCID: PMC11290206
- DOI: 10.1186/s12931-024-02916-w
Nephrectomy and high-salt diet inducing pulmonary hypertension and kidney damage by increasing Ang II concentration in rats
Abstract
Background: Chronic kidney disease (CKD) is a significant risk factor for pulmonary hypertension (PH), a complication that adversely affects patient prognosis. However, the mechanisms underlying this association remain poorly understood. A major obstacle to progress in this field is the lack of a reliable animal model replicating CKD-PH.
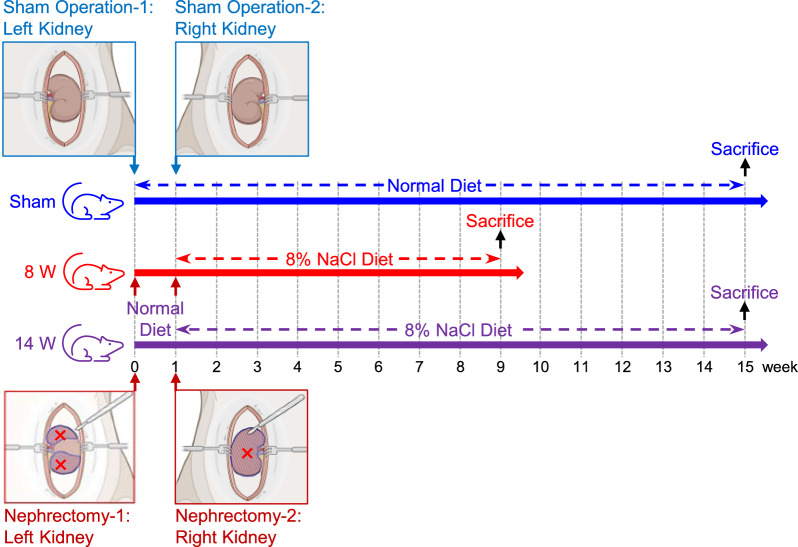
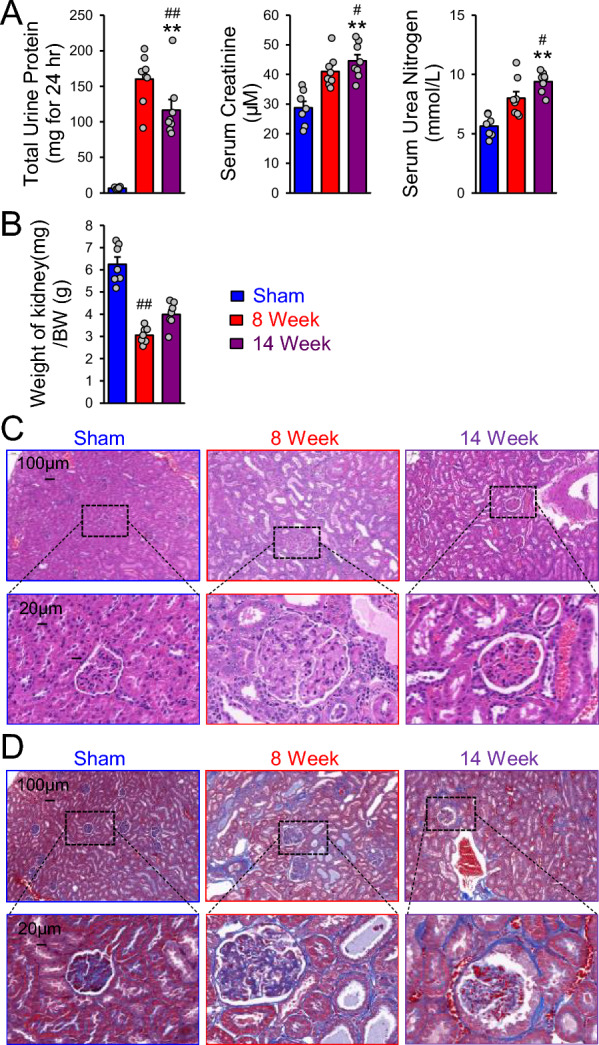
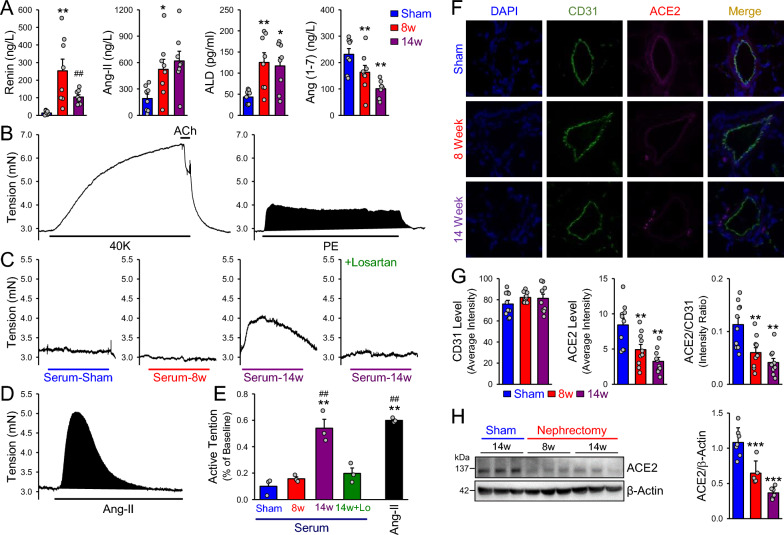
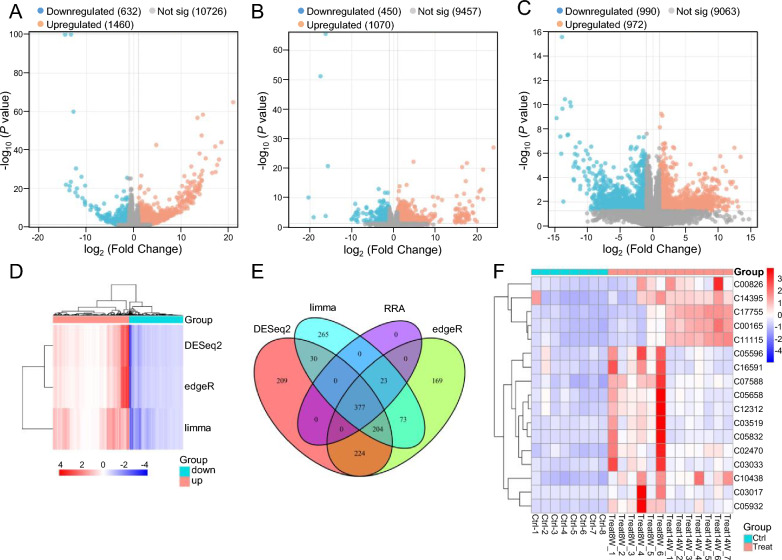
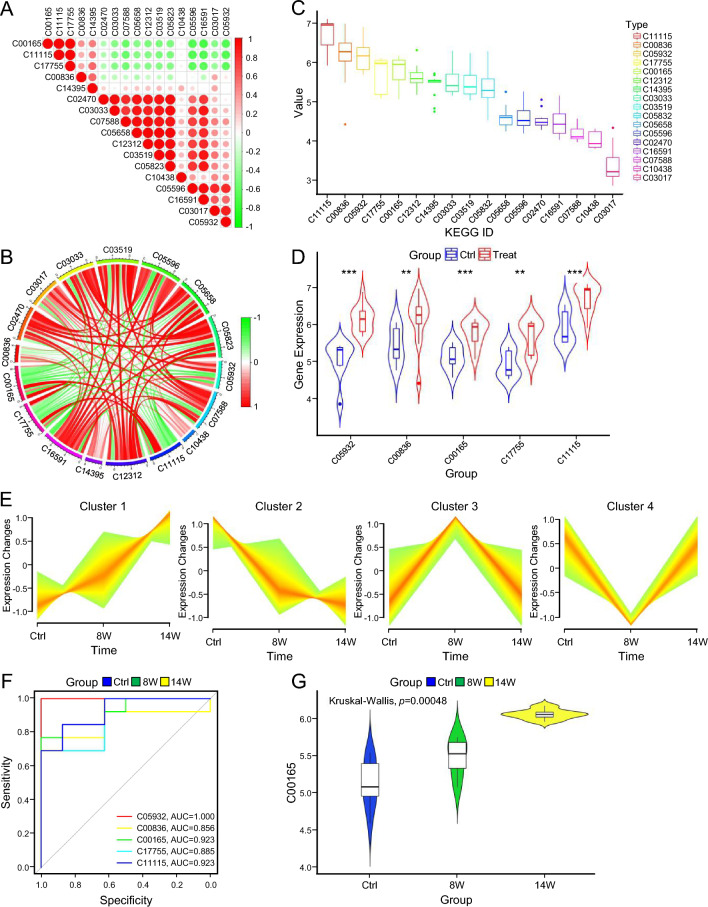
Methods: This study aimed to establish a stable rat model of CKD-PH. We employed a combined approach, inducing CKD through a 5/6 nephrectomy and concurrently exposing the rats to a high-salt diet. The model's hemodynamics were evaluated dynamically, alongside a comprehensive assessment of pathological changes in multiple organs. Lung tissues and serum samples were collected from the CKD-PH rats to analyze the expression of angiotensin-converting enzyme 2 (ACE2), evaluate the activity of key vascular components within the renin-angiotensin-aldosterone system (RAAS), and characterize alterations in the serum metabolic profile.
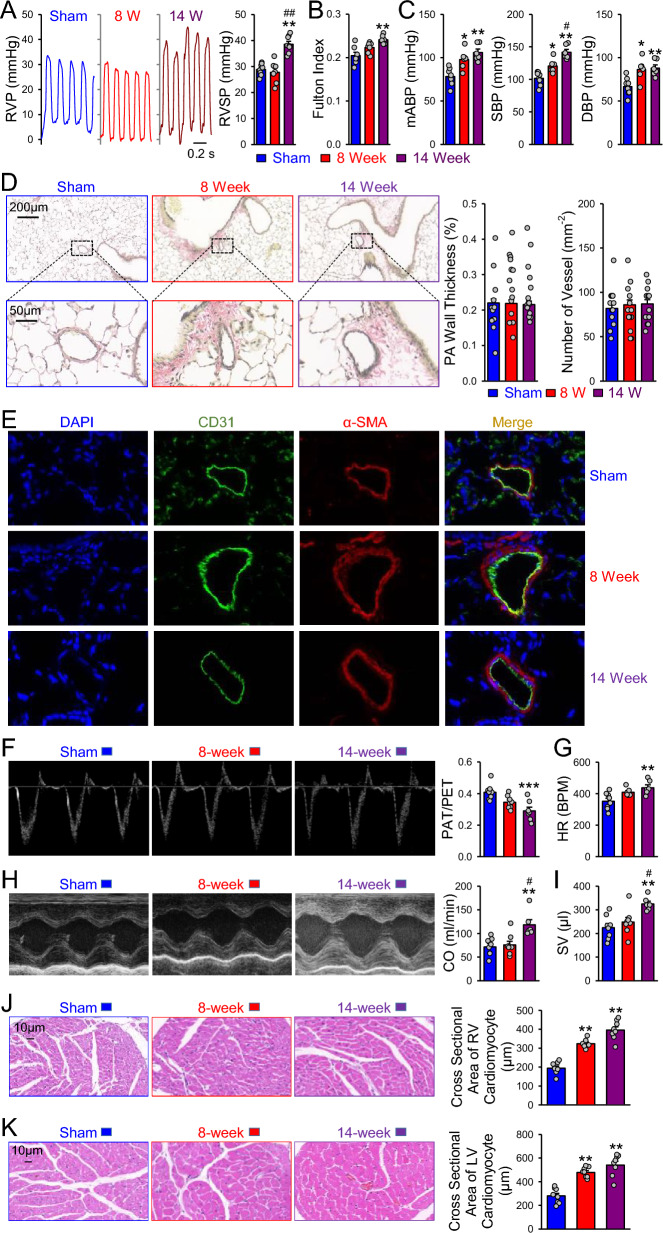
Results: At 14 weeks post-surgery, the CKD-PH rats displayed significant changes in hemodynamic parameters indicative of pulmonary arterial hypertension. Additionally, right ventricular hypertrophy was observed. Notably, no evidence of pulmonary vascular remodeling was found. Further analysis revealed RAAS dysregulation and downregulated ACE2 expression within the pulmonary vascular endothelium of CKD-PH rats. Moreover, the serum metabolic profile of these animals differed markedly from the sham surgery group.
Conclusions: Our findings suggest that the development of pulmonary arterial hypertension in CKD-PH rats is likely a consequence of a combined effect: RAAS dysregulation, decreased ACE2 expression in pulmonary vascular endothelial cells, and metabolic disturbances.
Keywords: Angiotensin converting enzyme 2; Chronic kidney disease; Metabolomics; Pulmonary hypertension; Renin–angiotensin–aldosterone system.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Dietary salt modifies the blood pressure response to renin-angiotensin inhibition in experimental chronic kidney disease.Am J Physiol Renal Physiol. 2021 Apr 1;320(4):F654-F668. doi: 10.1152/ajprenal.00603.2020. Epub 2021 Feb 15. Am J Physiol Renal Physiol. 2021. PMID: 33586496
-
Renin inhibition ameliorates renal damage through prominent suppression of both angiotensin I and II in human renin angiotensinogen transgenic mice with high salt loading.Clin Exp Nephrol. 2014 Aug;18(4):593-9. doi: 10.1007/s10157-013-0893-6. Epub 2013 Oct 24. Clin Exp Nephrol. 2014. PMID: 24154707
-
ACE2 activation confers endothelial protection and attenuates neointimal lesions in prevention of severe pulmonary arterial hypertension in rats.Lung. 2013 Aug;191(4):327-36. doi: 10.1007/s00408-013-9470-8. Epub 2013 May 8. Lung. 2013. PMID: 23652350
-
Hypertension: renin-angiotensin-aldosterone system alterations.Circ Res. 2015 Mar 13;116(6):960-75. doi: 10.1161/CIRCRESAHA.116.303587. Circ Res. 2015. PMID: 25767283 Review.
-
Comparison of the surgical resection and infarct 5/6 nephrectomy rat models of chronic kidney disease.Am J Physiol Renal Physiol. 2022 Jun 1;322(6):F639-F654. doi: 10.1152/ajprenal.00398.2021. Epub 2022 Apr 4. Am J Physiol Renal Physiol. 2022. PMID: 35379002 Free PMC article. Review.
References
-
- Selvaraj S, et al. Pulmonary hypertension is associated with a higher risk of heart failure hospitalization and mortality in patients with chronic kidney disease: the jackson heart study. Circ Heart Failure. 2017. 10.1161/circheartfailure.116.003940. 10.1161/circheartfailure.116.003940 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
