

Extranodal natural killer/T-cell lymphoma with tonsil involvement: a case report
- PMID: 39080655
- PMCID: PMC11290306
- DOI: 10.1186/s12903-024-04452-x
Extranodal natural killer/T-cell lymphoma with tonsil involvement: a case report
Abstract
Background: Extranodal natural killer/T-cell lymphoma (ENKTL) with tonsil involvement is not common, especially in children.
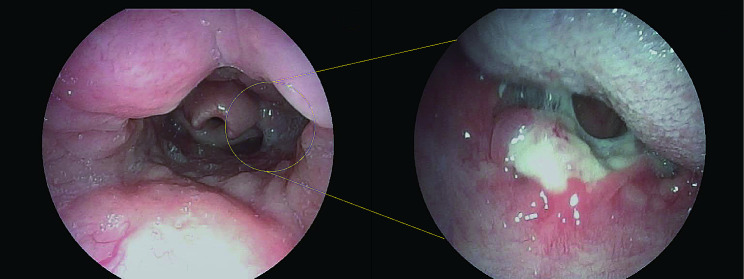
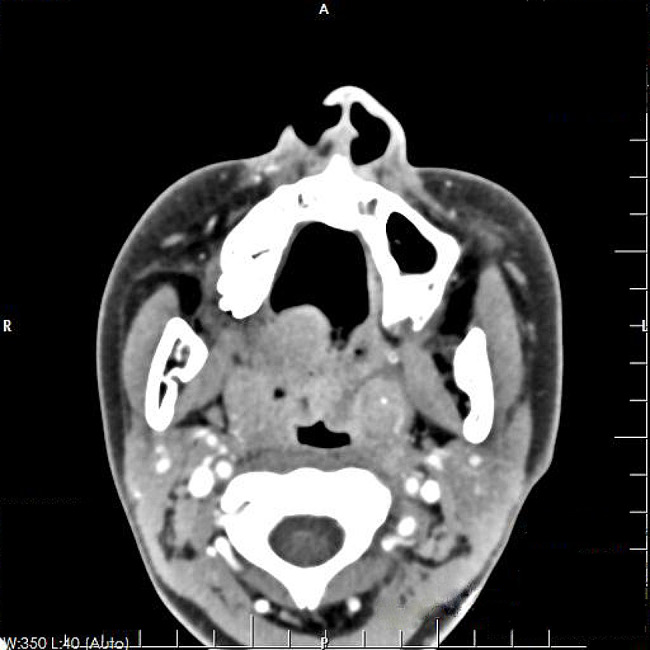
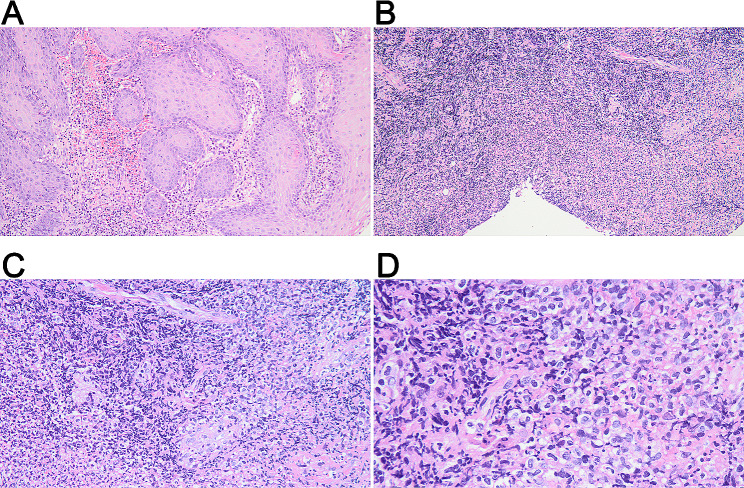
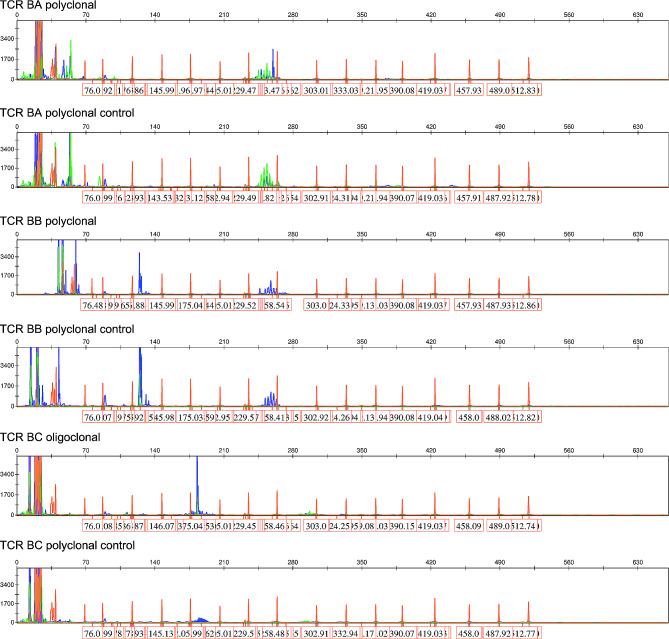
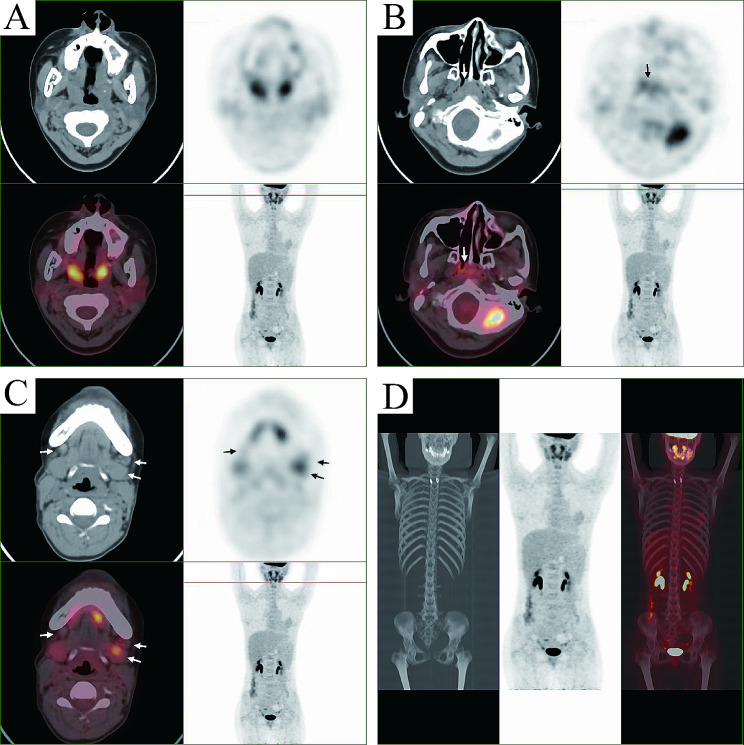
Case presentation: A 13-year-old girl presented with an unexplained sore throat for more than 2 months, together with intermittent fever and suppurative tonsilitis. Nasopharyngoscopy revealed a pharyngeal mass. Enhanced computed tomography (CT) scan showed tonsillar hypertrophy and punctate calcification. Chronic pyogenic granulomatous inflammation with pseudoepithelial squamous epithelial hyperplasia was observed in left tonsil, and pyogenic granulomatous inflammation and a small number of T-lymphoid cells were detected in the right tonsil. The immunohistochemical results showed CD2+, CD3+, CD4+, CD5+, CD8+, granzyme B+, and TIA-1+. The Ki-67 proliferation index was 20%. The case showed T cell receptor gene rearrangement. Finally, the case was diagnosed as ENKTL of stage II with tonsil involvement. The patient received 6 cycles of chemotherapy with SMILE regimen, and showed complete response with no recurrence in the follow-up.
Conclusion: We presented a rare case of ENKTL with tonsil involvement in a child. The patient showed complete response to the SMILE chemotherapy with no recurrence.
Keywords: Case report; ENKTL; Natural killer/T-cell lymphoma; SMILE chemotherapy; Tonsils.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Locke FL, Ghobadi A, Jacobson CA, Miklos DB, Lekakis LJ, Oluwole OO, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1–2 trial. Lancet Oncol. 2019;20(1):31–42. 10.1016/s1470-2045(18)30864-7. 10.1016/s1470-2045(18)30864-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
