

Mechanical versus manual cardiopulmonary resuscitation (CPR): an umbrella review of contemporary systematic reviews and more
- PMID: 39080740
- PMCID: PMC11290300
- DOI: 10.1186/s13054-024-05037-4
Mechanical versus manual cardiopulmonary resuscitation (CPR): an umbrella review of contemporary systematic reviews and more
Abstract
Background: High-quality cardiopulmonary resuscitation (CPR) can restore spontaneous circulation (ROSC) and neurological function and save lives. We conducted an umbrella review, including previously published systematic reviews (SRs), that compared mechanical and manual CPR; after that, we performed a new SR of the original studies that were not included after the last published SR to provide a panoramic view of the existing evidence on the effectiveness of CPR methods.
Methods: PubMed, EMBASE, and Medline were searched, including English in-hospital (IHCA) and out-of-hospital cardiac arrest (OHCA) SRs, and comparing mechanical versus manual CPR. A Measurement Tool to Assess Systematic Reviews (AMSTAR-2) and GRADE were used to assess the quality of included SRs/studies. We included both IHCA and OHCA, which compared mechanical and manual CPR. We analyzed at least one of the outcomes of interest, including ROSC, survival to hospital admission, survival to hospital discharge, 30-day survival, and survival to hospital discharge with good neurological function. Furthermore, subgroup analyses were performed for age, gender, initial rhythm, arrest location, and type of CPR devices.
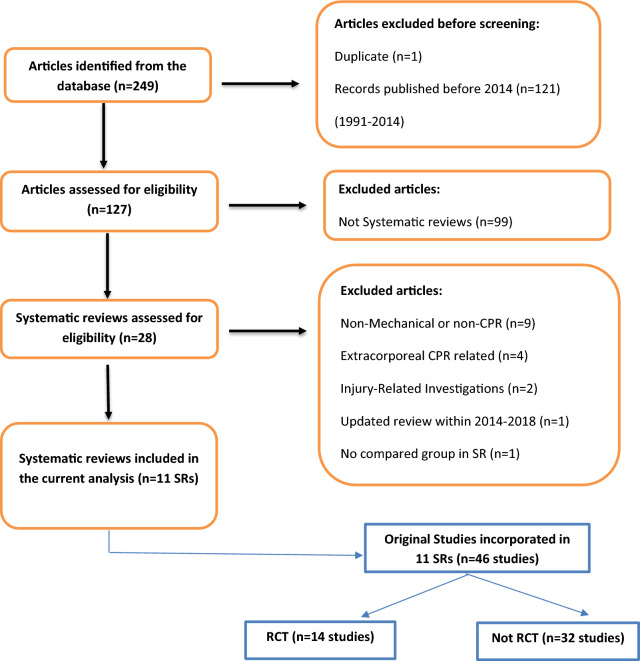
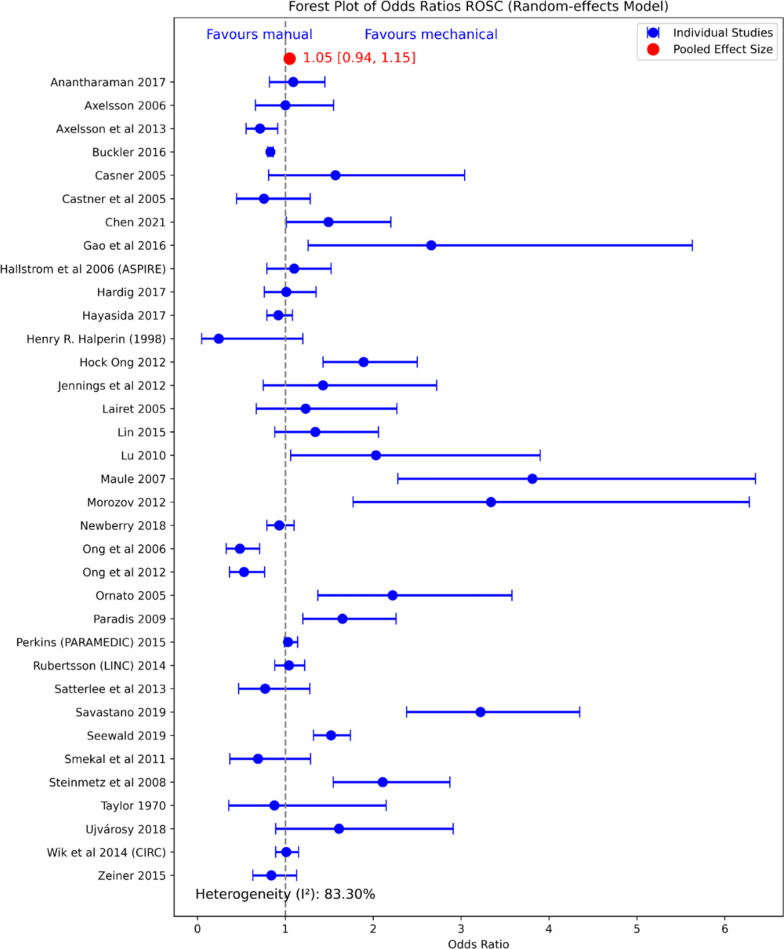
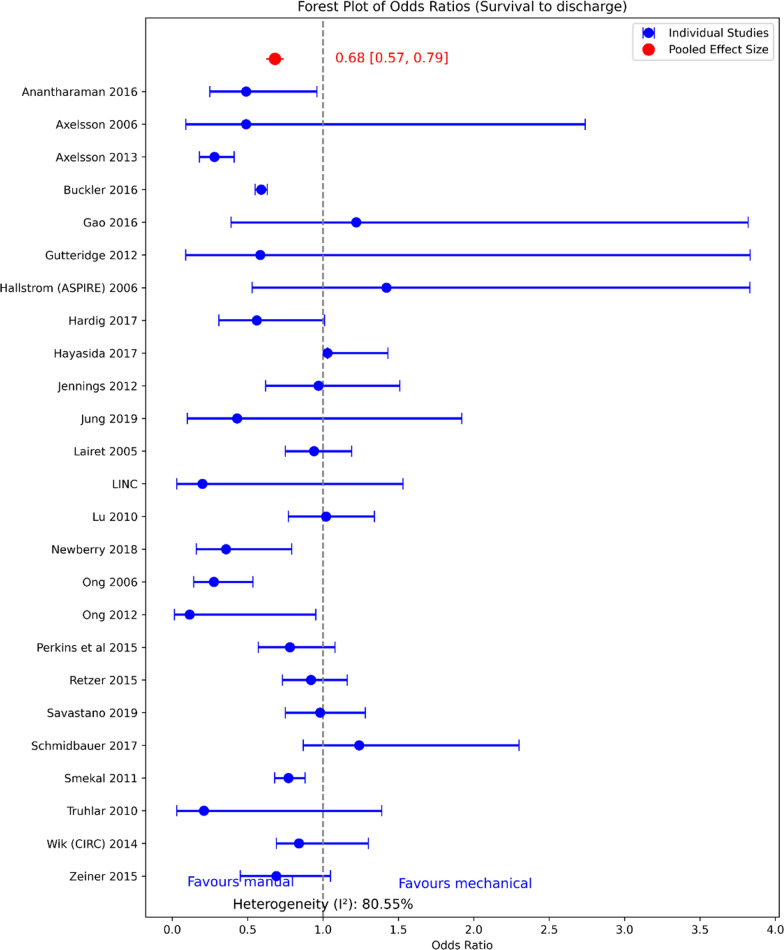
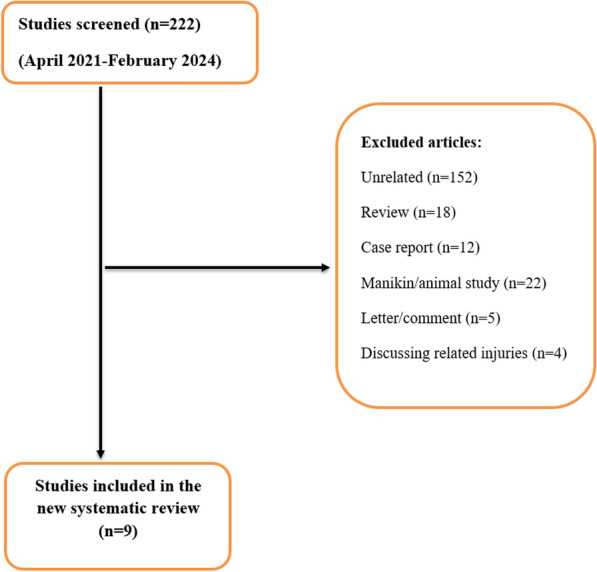
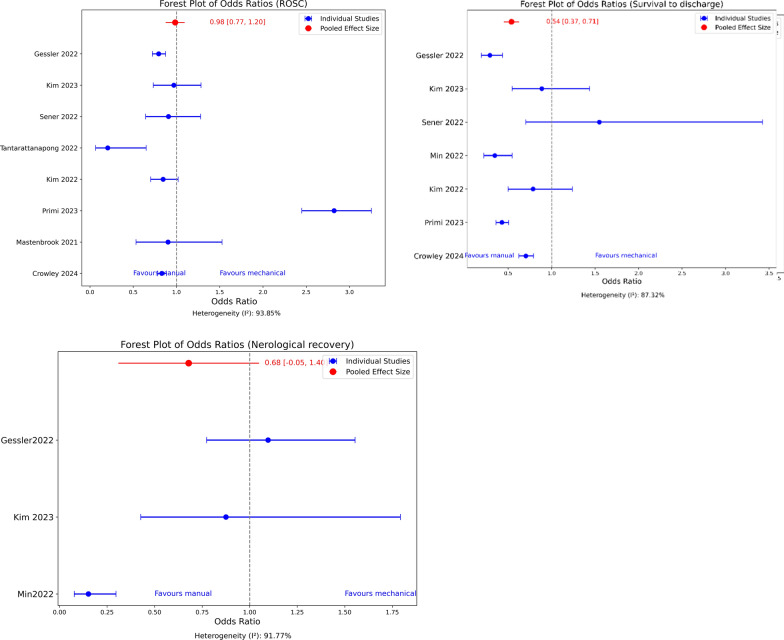
Results: We identified 249 potentially relevant records, of which 238 were excluded. Eleven SRs were analyzed in the Umbrella review (January 2014-March 2022). Furthermore, for a new, additional SR, we identified eight eligible studies (not included in any prior SR) for an in-depth analysis between April 1, 2021, and February 15, 2024. The higher chances of using mechanical CPR for male patients were significantly observed in three studies. Two studies showed that younger patients received more mechanical treatment than older patients. However, studies did not comment on the outcomes based on the patient's gender or age. Most SRs and studies were of low to moderate quality. The pooled findings did not show the superiority of mechanical compared to manual CPR except in a few selected subgroups.
Conclusions: Given the significant heterogeneity and methodological limitations of the included studies and SRs, our findings do not provide definitive evidence to support the superiority of mechanical CPR over manual CPR. However, mechanical CPR can serve better where high-quality manual CPR cannot be performed in selected situations.
Keywords: CPR; Cardiac arrest; IHCA; Manual CPR; Mechanical CPR; OHCA; ROSC; Survival.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Comparison of mechanical versus manual cardiopulmonary resuscitation in cardiac arrest.Crit Care. 2024 Sep 27;28(1):319. doi: 10.1186/s13054-024-05088-7. Crit Care. 2024. PMID: 39334247 Free PMC article. No abstract available.
-
An update on the mechanical versus manual cardiopulmonary resuscitation in cardiac arrest patients.Crit Care. 2024 Oct 22;28(1):340. doi: 10.1186/s13054-024-05131-7. Crit Care. 2024. PMID: 39438999 Free PMC article. No abstract available.
References
-
- Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81(11):1479–87. 10.1016/j.resuscitation.2010.08.006. - PubMed
-
- Gräsner JT, Herlitz J, Tjelmeland IBM, Wnent J, Masterson S, Lilja G, Bein B, Böttiger BW, Rosell-Ortiz F, Nolan JP, Bossaert L, Perkins GD. European resuscitation council guidelines 2021: epidemiology of cardiac arrest in Europe. Resuscitation. 2021;161:61–79. - PubMed
-
- Aune S, Herlitz J, Bang A. Characteristics of patients who die in hospital with no attempt at resuscitation. Resuscitation. 2005;65:291–9. - PubMed
-
- Bergum D, Nordseth T, Mjolstad OC, Skogvoll E, Haugen BO. Causes of in-hospital cardiac arrest: incidences and rate of recognition. Resuscitation. 2015;87:63–8. - PubMed
-
- Randhawa VK, Grunau BE, Debicki DB, Zhou J, Hegazy AF, McPherson T, Nagpal AD. Cardiac Intensive Care Unit management of patients after cardiac arrest: now the real work begins. Can J Cardiol. 2018;34(2):156–67. 10.1016/j.cjca.2017.11.013. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
