

Opioid exit plans for tapering postoperative pain control in noncancer patients: a systematic review
- PMID: 39080780
- PMCID: PMC11290124
- DOI: 10.1186/s13037-024-00408-w
Opioid exit plans for tapering postoperative pain control in noncancer patients: a systematic review
Abstract
Background: A growing number of countries have reported sharp increases in the use and harm of opioid analgesics. High rates of new opioid initiation are observed in postoperative patients. In response, various tertiary care institutions have developed opioid exit plans (OEPs) to curb potential opioid-related harm.
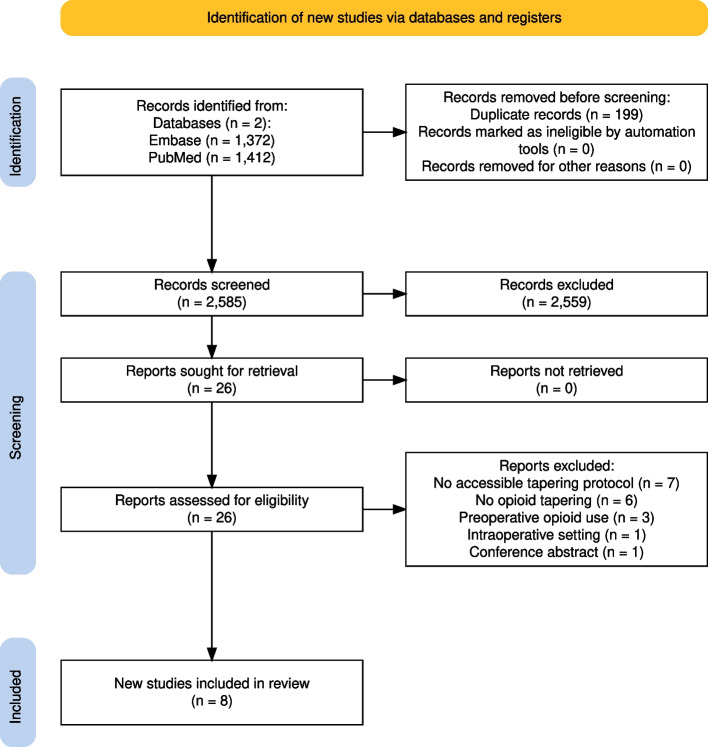
Methods: PubMed and Embase were systematically searched to identify, summarize, and compare the interventional elements of OEPs for postoperative patient populations published from January 1, 2000, to June 4, 2024. Two researchers independently screened the articles for eligibility following the PRISMA 2020 guidelines, extracted the data, and assessed the study quality and risk of bias. Data synthesis was performed for study characteristics, intervention details, efficacy, and development.
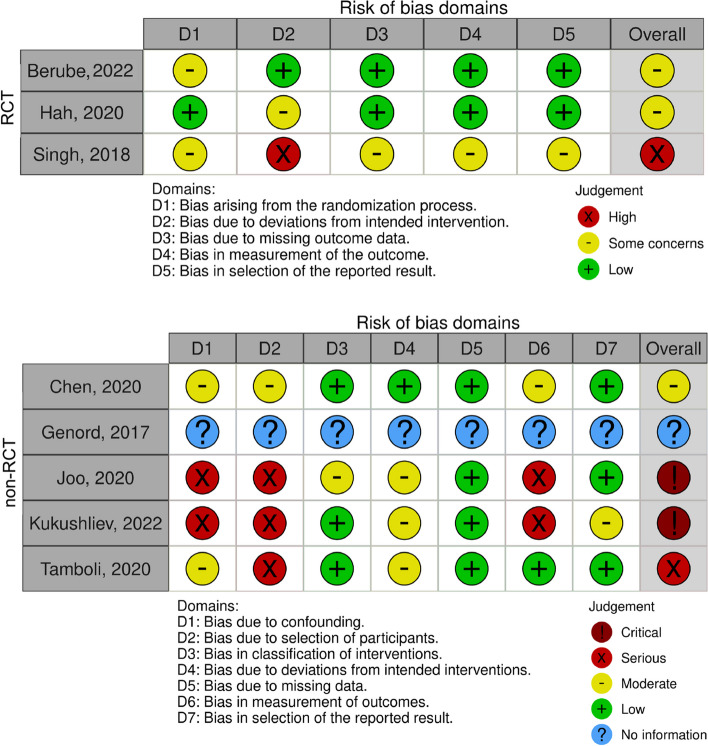
Results: A total of 2,585 articles were screened, eight of which met the eligibility criteria. All studies were conducted in North America and focused on orthopedic surgery patients following total hip or knee arthroplasty (n = 5) or neurosurgery (n = 3). Most studies (n = 7) included a pre-post (n = 4) or randomized clinical design (n = 3). Three studies were of good quality, and none had a low risk of bias. The interventions varied and ranged from educational sessions (n = 1) to individualized tapering protocols (n = 4) or a combination of the two (n = 2). Key elements were instructions on how to anticipate patients' postoperative need for opioid analgesics and tapering strategies based on 24-h predischarge opioid consumption. Six studies included efficacy as an endpoint in their analysis, of which four assessed statistical significance, with all four identifying that the OEPs were successful in reducing postoperative opioid use.
Conclusion: Despite differences in design and implementation, the identified OEPs suggest that they are efficacious in reducing outpatient opioid consumption. They provide a robust estimate of postoperative analgesic requirements and a rationale for tapering duration and rate. However, more rigorous studies are needed to evaluate their real-world effectiveness.
Keywords: Deprescribing; Drug safety; Hospital discharge; Noncancer pain; Opioid analgesics; Opioid tapering; Postoperative patient management; Preventive medicine; Systematic review; Transitional care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Spencer M, Miniño A, Warner M. Drug Overdose Deaths in the United States, 2001–2021 [Internet]. National Center for Health Statistics (U.S.); 2022 [cited 2023 Oct 24]. Available from: https://stacks.cdc.gov/view/cdc/122556
-
- Understanding the Opioid Overdose Epidemic [Internet]. Center for Disease Control and Prevention; 2021 [cited 2023 Oct 24]. Available from: https://www.cdc.gov/opioids/basics/epidemic.html
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
