

Utility of laryngeal electromyography for establishing prognosis and individualized treatment after laryngeal neuropathies
- PMID: 39080992
- PMCID: PMC11998967
- DOI: 10.1002/mus.28207
Utility of laryngeal electromyography for establishing prognosis and individualized treatment after laryngeal neuropathies
Abstract
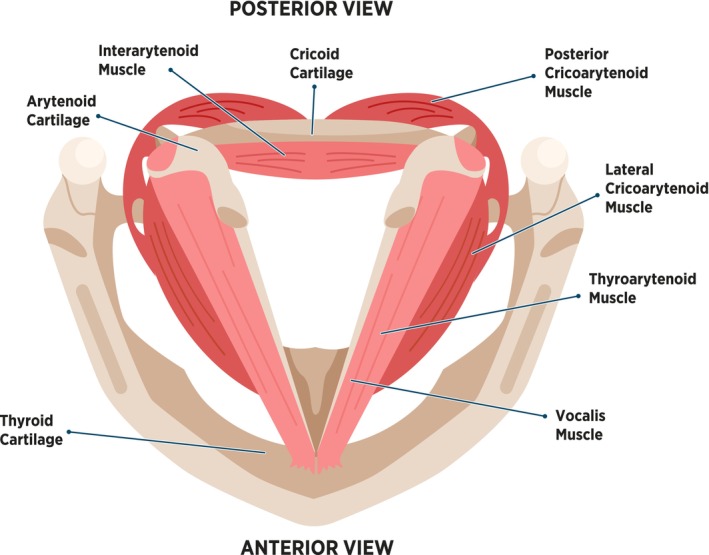
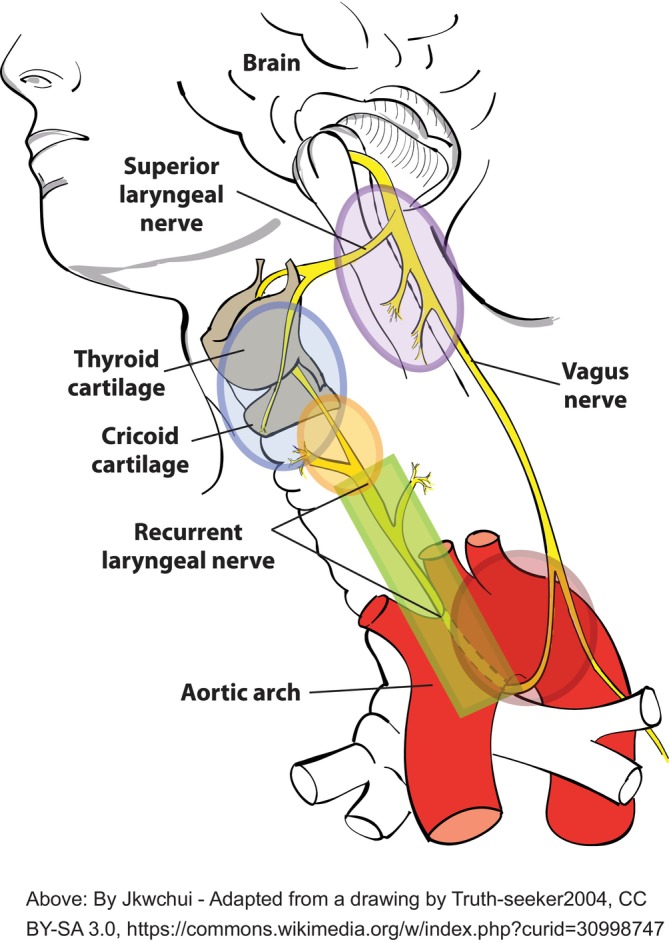
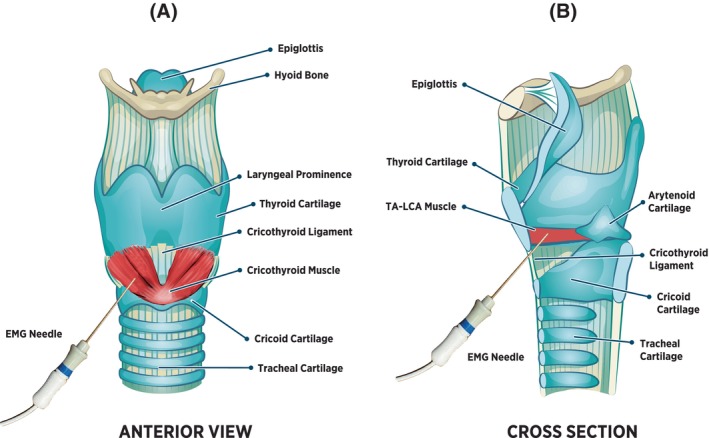
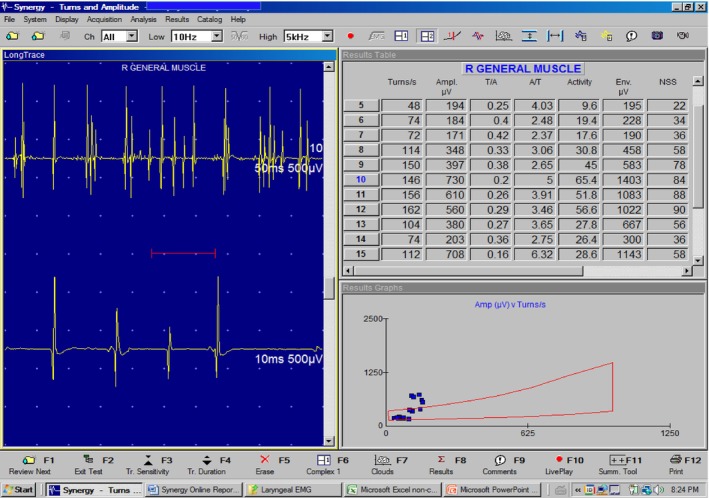
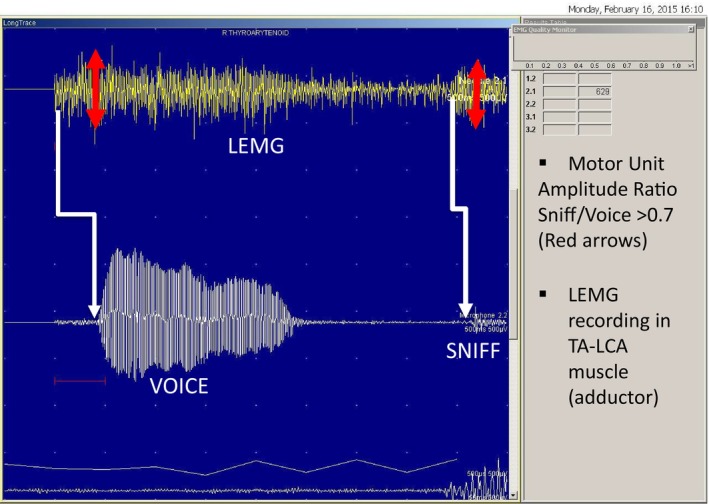
Laryngeal electromyography (LEMG) is a technique used to characterize neuropathic injuries to the recurrent laryngeal nerve (RLN) and superior laryngeal nerve (SLN). The RLN and SLN innervate the laryngeal muscles to produce vocal fold (VF) motion and elongation, respectively. VF motion deficiencies can affect voice, swallowing, and breathing, which can greatly affect a patient's quality of life. Neuropathy-related VF motion deficiencies most often result from surgical interventions to the skull base, neck, or chest likely due to the circuitous route of the RLN. LEMG is ideally conducted by an electromyographer and an otolaryngologist using a team-approach. LEMG is a powerful diagnostic tool to better characterize the extent of neuropathic injury and thus clarify the prognosis for VF motion recovery. This updated review discusses current techniques to improve the positive and negative predictive values of LEMG using laryngeal synkinesis and quantitative LEMG. Synkinesis can be diagnosed by comparing motor unit potential amplitude during vocalization and sniff maneuvers when recording within adductor muscles. Quantitative turns analysis can measure motor unit recruitment to avoid subjective descriptions of reduced depolarization during vocalization, and normal values are >400 turns/s. By integrating qualitative, quantitative, and synkinetic data, a robust prognosis can help clinicians determine if VF weakness will recover. Based on LEMG interpretation, patient-centered treatment can be developed to include watchful waiting, temporary VF augmentation, or definitive medialization procedures and laryngeal reinnervation.
Keywords: nerve injury; peripheral nerve injury; recurrent laryngeal nerve; superior laryngeal nerve.
© 2024 The Author(s). Muscle & Nerve published by Wiley Periodicals LLC.
Conflict of interest statement
Dr. Smith is on the advisory board for Inovio Pharmaceuticals but no conflicts with this review. Dr. Munin declares research support from Abbvie, Merz, and Ipsen and consulting with Pacira but no conflicts with this review.
Figures
Similar articles
-
The properties of laryngeal electromyography in the non-paralyzed sides of patients with idiopathic vocal cord paralysis.Eur Arch Otorhinolaryngol. 2025 Feb;282(2):927-936. doi: 10.1007/s00405-024-09116-8. Epub 2024 Dec 7. Eur Arch Otorhinolaryngol. 2025. PMID: 39643814
-
Innervation status in chronic vocal fold paralysis and implications for laryngeal reinnervation.Laryngoscope. 2018 Jul;128(7):1628-1633. doi: 10.1002/lary.27078. Epub 2018 Jan 22. Laryngoscope. 2018. PMID: 29355973
-
Electromyographic laryngeal synkinesis alters prognosis in vocal fold paralysis.Laryngoscope. 2010 Feb;120(2):285-90. doi: 10.1002/lary.20629. Laryngoscope. 2010. PMID: 19950370
-
Unilateral recurrent laryngeal nerve paralysis.J Voice. 1994 Mar;8(1):79-83. doi: 10.1016/s0892-1997(05)80323-6. J Voice. 1994. PMID: 8167791 Review.
-
Laryngeal Electromyography.Adv Otorhinolaryngol. 2020;85:18-24. doi: 10.1159/000456680. Epub 2020 Nov 9. Adv Otorhinolaryngol. 2020. PMID: 33166978 Review.
References
-
- Weddell G, Feinstein B, Pattle RE. The electrical activity of voluntary muscle in man under normal and pathological conditions. Brain. 1944;67:178‐257.
-
- Galen C. Galen: On Anatomical Procedures, The Later Books. Translated by W.L.H. Duckworth. The University Press; 1962.
-
- Galen C. Galen on the Usefulness of the Parts of the Body. Translated by M.T. May. Vol I. Cornell University Press; 1968.
-
- Onodi A. Die Anatomie und Physiologie der Kehlkopfnerven. Oscar Coblentz, 1902.
-
- Lemiere F. Innervation of the larynx: innervation of the laryngeal muscles. Am J Anat. 1932;31:417‐438.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
