

Efficacy and Safety of Lumasiran in Patients With Primary Hyperoxaluria Type 1: Results from a Phase III Clinical Trial
- PMID: 39081738
- PMCID: PMC11284403
- DOI: 10.1016/j.ekir.2024.04.048
Efficacy and Safety of Lumasiran in Patients With Primary Hyperoxaluria Type 1: Results from a Phase III Clinical Trial
Abstract
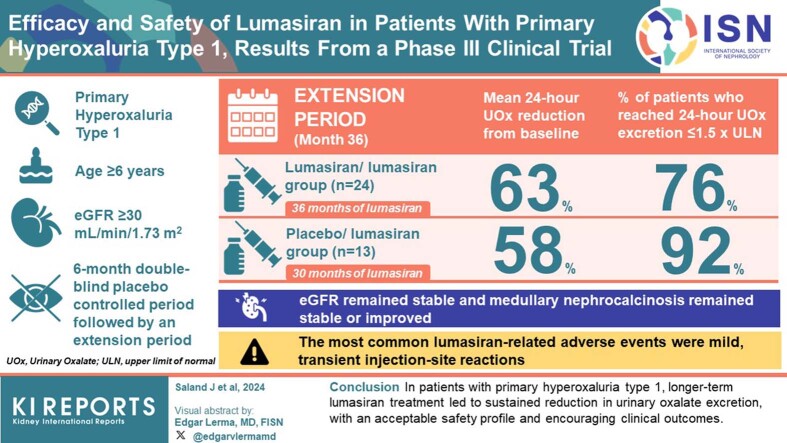
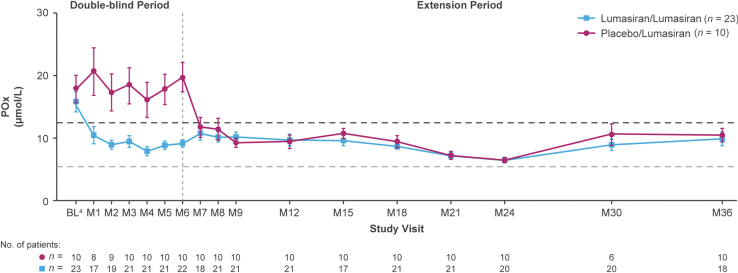
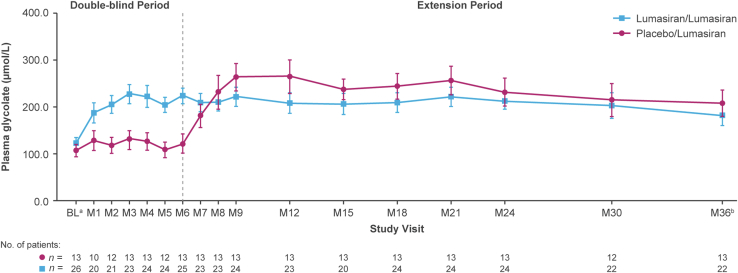
Introduction: Patients with primary hyperoxaluria type 1 (PH1), a genetic disorder associated with hepatic oxalate overproduction, frequently experience recurrent kidney stones and worsening kidney function. Lumasiran is indicated for the treatment of PH1 to lower urinary and plasma oxalate (POx).
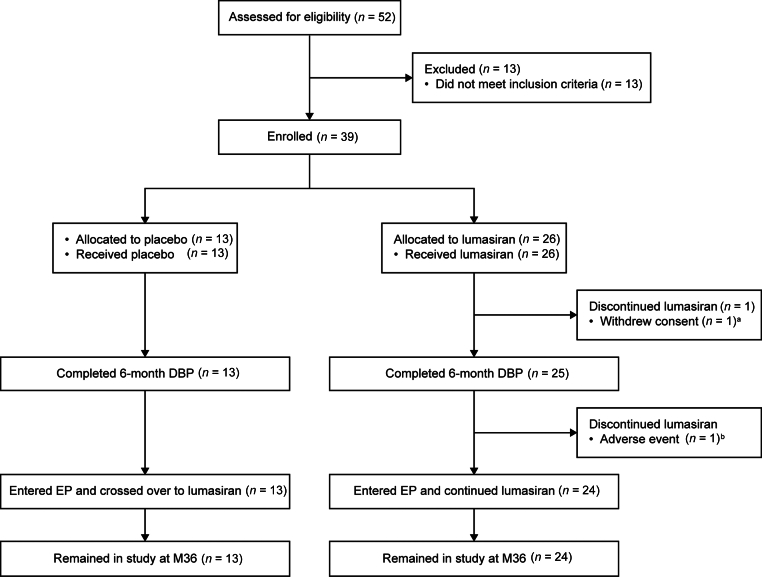
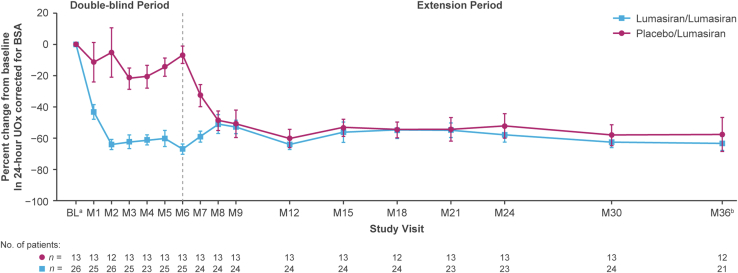
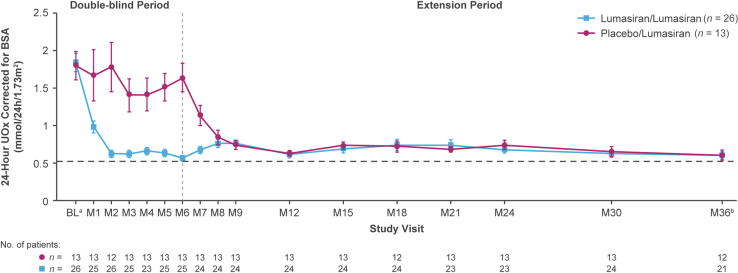
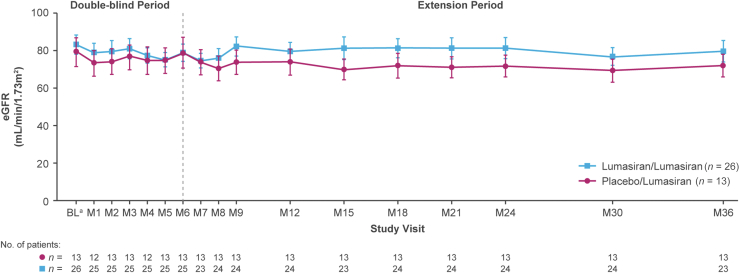
Methods: ILLUMINATE-A (NCT03681184) is a phase III trial in patients aged ≥6 years with PH1 and estimated glomerular filtration rate (eGFR) ≥30 ml/min per 1.73 m2. A 6-month double-blind placebo-controlled period is followed by an extension period (≤54 months; all patients receive lumasiran). We report interim data through month 36.
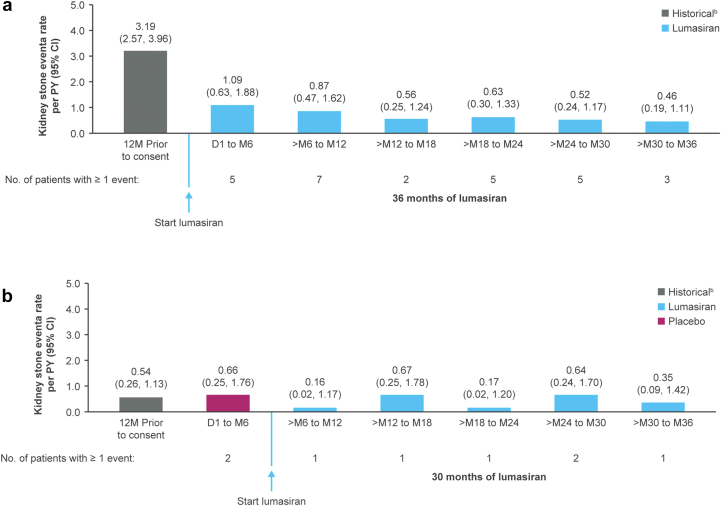
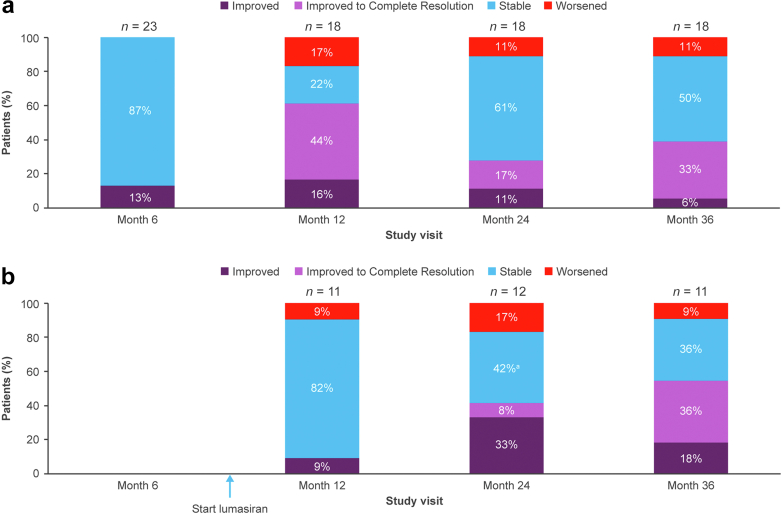
Results: Of 39 patients enrolled, 24 of 26 (lumasiran/lumasiran group) and 13 of 13 (placebo/lumasiran group) entered and continue in the extension period. At month 36, in the lumasiran/lumasiran group (36 months of lumasiran treatment) and placebo/lumasiran group (30 months of lumasiran treatment), mean 24-hour urinary oxalate (UOx) reductions from baseline were 63% and 58%, respectively; 76% and 92% of patients reached a 24-hour UOx excretion ≤1.5× the upper limit of normal (ULN). eGFR remained stable. Kidney stone event rates decreased from 2.31 (95% confidence interval: 1.88-2.84) per person-year (PY) during the 12 months before consent to 0.60 (0.46-0.77) per PY during lumasiran treatment. Medullary nephrocalcinosis generally remained stable or improved; approximately one-third of patients (both groups) improved to complete resolution. The most common lumasiran-related adverse events (AEs) were mild, transient injection-site reactions.
Conclusion: In patients with PH1, longer-term lumasiran treatment led to sustained reduction in UOx excretion, with an acceptable safety profile and encouraging clinical outcomes.See for Video Abstract.
Keywords: RNA interference; lumasiran; oxalate; primary hyperoxaluria type 1; rare disease; renal.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
