

Venetoclax-obinutuzumab for previously untreated chronic lymphocytic leukemia: 6-year results of the randomized phase 3 CLL14 study
- PMID: 39082668
- PMCID: PMC11551846
- DOI: 10.1182/blood.2024024631
Venetoclax-obinutuzumab for previously untreated chronic lymphocytic leukemia: 6-year results of the randomized phase 3 CLL14 study
Abstract
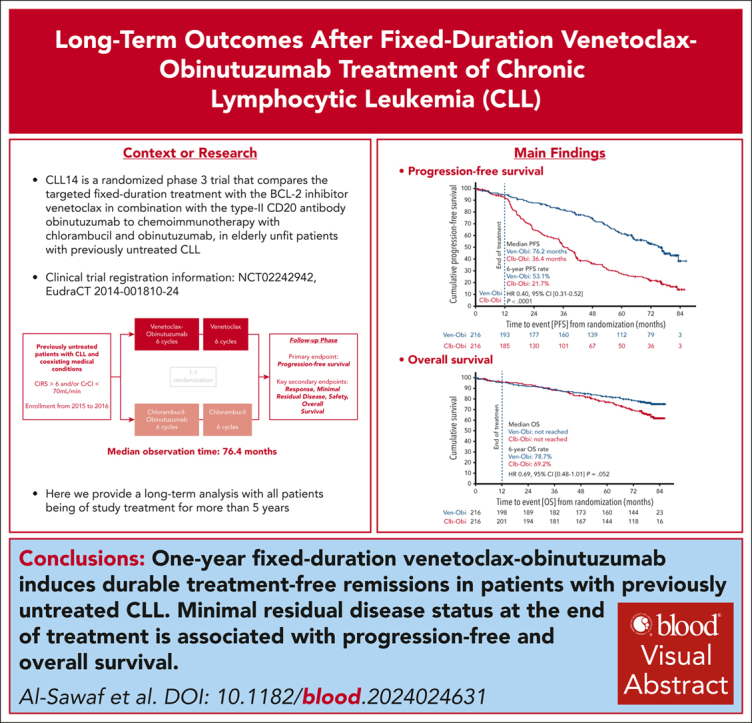
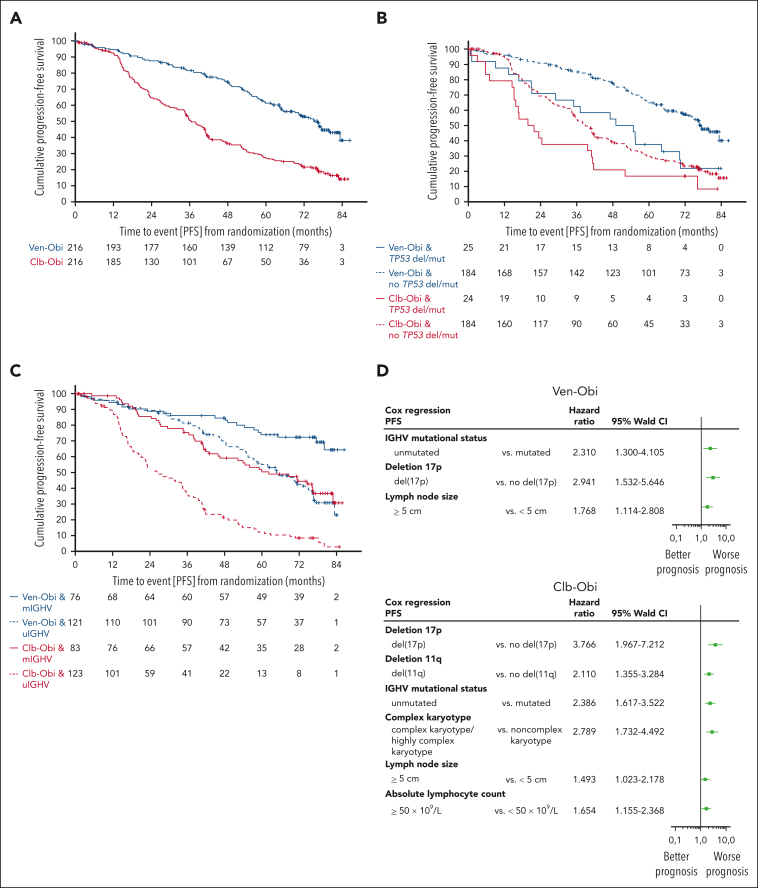
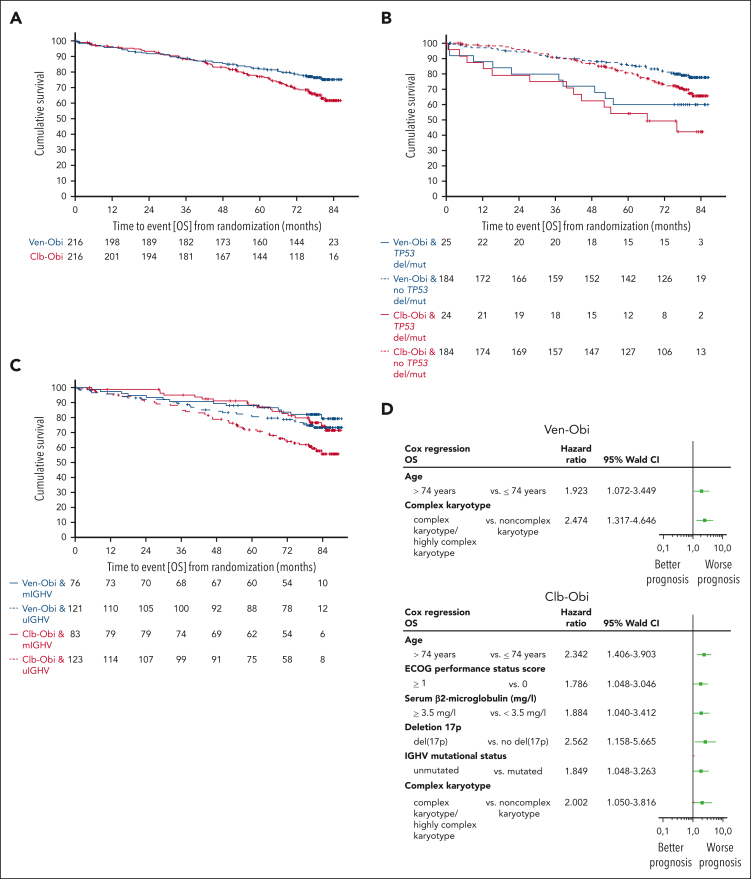
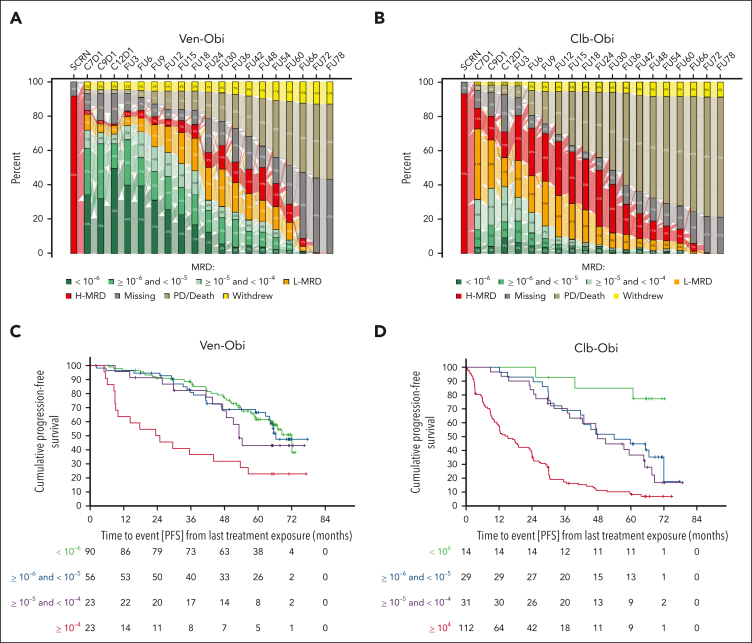
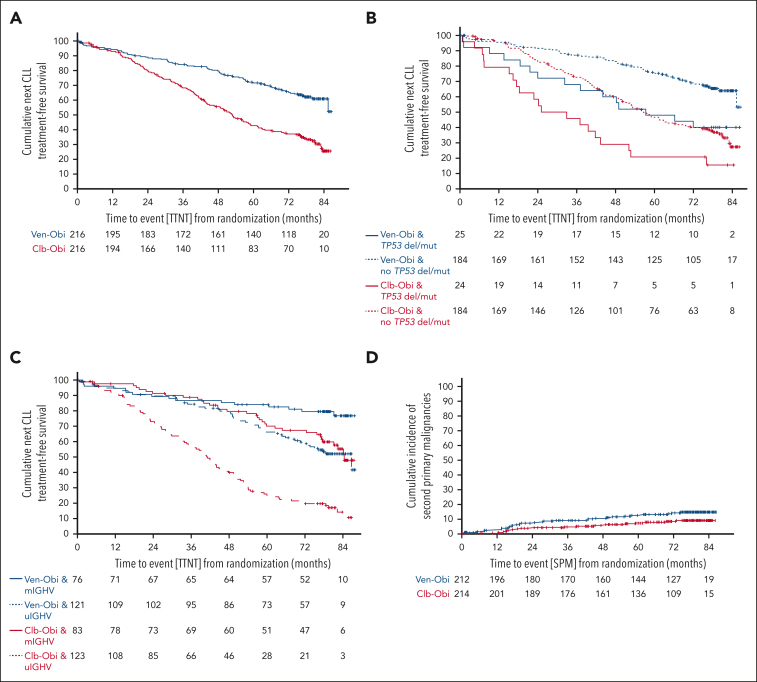
In the CLL14 study, patients with previously untreated chronic lymphocytic leukemia (CLL) and coexisting conditions were randomized to 12 cycles of venetoclax-obinutuzumab (Ven-Obi, n = 216) or chlorambucil-obinutuzumab (Clb-Obi, n = 216). Progression-free survival (PFS) was the primary end point. Key secondary end points included time-to-next-treatment (TTNT), rates of undetectable minimal residual disease (uMRD), overall survival (OS), and rates of adverse events. Patient reported outcomes of time until definitive deterioration (TUDD) in quality of life (QoL) were analyzed. At a median observation time of 76.4 months, PFS remained superior for Ven-Obi compared with Clb-Obi (median, 76.2 vs 36.4 months; hazard ratio [HR], 0.40; 95% confidence interval [CI], 0.31-0.52; P < .0001). Likewise, TTNT was longer after Ven-Obi (6-year TTNT, 65.2% vs 37.1%; HR, 0.44; 95% CI, 0.33-0.58; P < .0001). In the Ven-Obi arm, presence of del(17p), unmutated immunoglobulin heavy-chain variable region, and lymph node size of ≥5 cm were independent prognostic factors for shorter PFS. The 6-year OS rate was 78.7% in the Ven-Obi and 69.2% in the Clb-Obi arm (HR, 0.69; 95% CI, 0.48-1.01; P = .052). A significantly longer TUDD in global health status/QoL was observed in the Ven-Obi than in the Clb-Obi arm (median, 82.1 vs 65.1 months; HR, 0.70; 95% CI, 0.51-0.97). Follow-up-adjusted second primary malignancies incidence rates were 2.3 and 1.4 per 1000 patient-months in the Ven-Obi and Clb-Obi arm, respectively. The sustained long-term survival and QoL benefits support the use of 1-year fixed-duration Ven-Obi in CLL. This trial was registered at www.ClinicalTrials.gov as #NCT02242942.
© 2024 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: O.A.-S. reports advisory board participation with Ascentage, AstraZeneca, AbbVie, Gilead, Janssen, and Roche; received speaker honoraria from Adaptive, AstraZeneca, AbbVie, BeiGene, Gilead, Janssen, and Roche; and received research funding from BeiGene, AbbVie, Janssen, and Roche). S.R. reports honoraria from Merck Shapre and Dohme (MSD). S.O., Y.M.C., J.D, M.B., and Y.J. report employment with Genentech/Hoffmann-la Roche. A.-M.F. reports personal fees from Celgene, Janssen, and Hoffmann-La Roche. E.T. reports advisory board participation with AbbVie, Janssen-Cilag, and BeiGene; received speaker honoraria from AstraZeneca, AbbVie, BeiGene, Gilead, Janssen, and Roche; and received research funding from Roche, AbbVie, and Gilead. C.S. received speaker honoraria from AstraZeneca and AbbVie; and reports advisory board participation with Janssen-Cilag). M.R. reports grants from F. Hoffman-La Roche Ltd; and personal fees from F. Hoffmann-La Roche Ltd and AbbVie. K.-A.K. reports grants from F. Hoffmann-La Roche Ltd and AbbVie, during the conduct of the study; and received personal fees from F. Hoffmann-La Roche Ltd and AbbVie. C.U.N. reports grants and/or consultancy fees from AbbVie, Janssen, AstraZeneca, BeiGene, Genmab, Octapharma, MSD, Lilly, Takeda, CSL Behring, and Novo Nordisk Foundation. B.C. reports employment with AbbVie. C.P.P. received speaker honoraria from AstraZeneca and Pfizer; reports research funding from Gilead Sciences; and reports advisory board participation with AbbVie. R.W. reports advisory board participation with AbbVie, BeiGene, and Janssen; reports speaker honoraria from AbbVie and Janssen; and received research funding from BioOra, and Janssen. J.P. reports employment with Genentech/Hoffmann-la Roche. B.E. reports grants and personal fees from F. Hoffmann-La Roche Ltd, AbbVie, AstraZeneca, BeiGene, and Janssen; reports personal fees from Celgene, Novartis, ArQule, Gilead, Oxford Biomedica (United Kingdom), Adaptive Biotechnologies, and Hexal. S.S. reports grants, personal fees, and nonfinancial support from AbbVie, AstraZeneca, Celgene, Gilead, GlaxoSmithKline, Hoffmann La-Roche Ltd, Janssen, Novartis, Pharmacyclics, Sunesis, and Verastem. Y.J. reports employment with Genentech/Hoffmann-La Roche; and reports stock in Genentech. M.H. received honoraria from Roche, Janssen, AbbVie, Gilead Sciences, and AstraZeneca; reports advisory or consulting role with Janssen, AbbVie, Gilead Sciences, Genentech/Roche, and AstraZeneca; participates in speakers bureau of Janssen, AbbVie, Gilead Sciences, Roche/Genentech, and AstraZeneca; reports research funding from Roche, AbbVie, Janssen, Gilead Sciences, and AstraZeneca; and received travel, accommodations, and expenses funds from Roche and Janssen. K.F reports advisory board participation with AstraZeneca and AbbVie; received speaker honoraria from AbbVie and Roche; and received research funding from AbbVie and Roche. The remaining authors declare no competing financial interests.
Figures
Comment in
-
Toward a new paradigm for CLL treatment.Blood. 2024 Oct 31;144(18):1849-1850. doi: 10.1182/blood.2024025896. Blood. 2024. PMID: 39480414 No abstract available.
References
-
- Hallek M, Al-Sawaf O. Chronic lymphocytic leukemia: 2022 update on diagnostic and therapeutic procedures. Am J Hematol. 2021;96(12):1679–1705. - PubMed
-
- Burger JA. Treatment of chronic lymphocytic leukemia. N Engl J Med. 2020;383(5):460–473. - PubMed
-
- Shadman M. Diagnosis and treatment of chronic lymphocytic leukemia: a review. JAMA. 2023;329(11):918–932. - PubMed
-
- Ashkenazi A, Fairbrother WJ, Leverson JD, Souers AJ. From basic apoptosis discoveries to advanced selective BCL-2 family inhibitors. Nat Rev Drug Discov. 2017;16(4):273–284. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
