

Electrical vagus nerve stimulation is a promising approach to reducing pulmonary complications after an esophagectomy: an experimental rodent model
- PMID: 39083131
- PMCID: PMC11618150
- DOI: 10.1007/s12026-024-09523-3
Electrical vagus nerve stimulation is a promising approach to reducing pulmonary complications after an esophagectomy: an experimental rodent model
Abstract
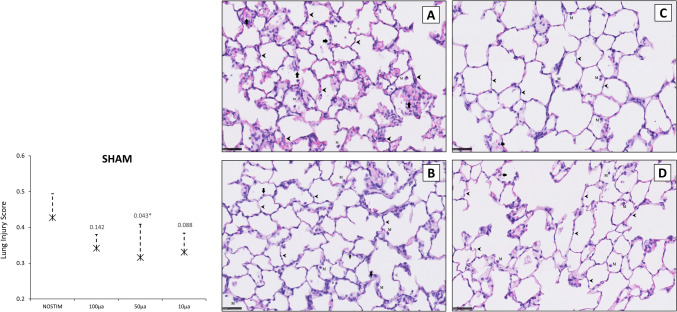
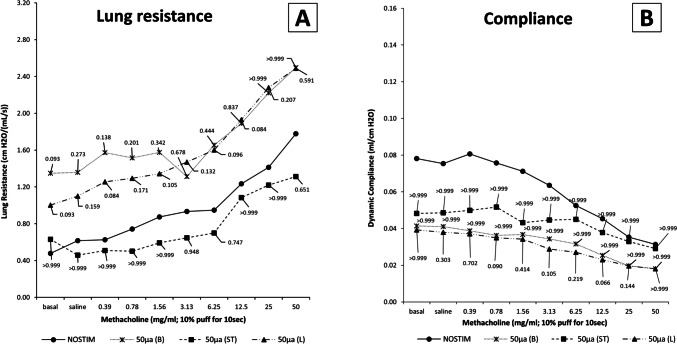
After esophagectomy, an imbalanced inflammatory response increases the risk of postoperative morbidity. The vagus nerve modulates local and systemic inflammatory responses, but its pulmonary branches are transected during esophagectomy as part of the oncological resection, which may account for the high incidence of postoperative (pulmonary) complications. This study investigated the effect of electrical vagus nerve stimulation (VNS) on lipopolysaccharide (LPS)-induced lung injury in rats. Rats (n = 60) were randomly assigned to a non-vagotomy or cervical vagotomy group, with VNS or without (NOSTIM). There were four non-vagotomy groups: NOSTIM and bilateral VNS with 100, 50, or 10 µA. The four vagotomy groups were NOSTIM and VNS with fixed amplitude (50 µA) bilaterally before (VNS-50-before) or after bilateral vagotomy (VNS-50-after), or unilaterally (left) before ipsilateral vagotomy (VNS-50-unilaterally). LPS was administered intratracheally after surgery. Pulmonary function, pro-inflammatory cytokines in serum, broncho-alveolar lavage fluid (BALF), and histopathological lung injury (LIS) were assessed 180 min post-procedure. In non-vagotomized rats, neutrophil influx in BALF following intra-tracheal LPS (mean 30 [± 23]; P = 0.075) and LIS (mean 0.342 [± 0.067]; P = 0.142) were similar after VNS-100, compared with NOSTIM. VNS-50 reduced neutrophil influx (23 [± 19]; P = 0.024) and LIS (0.316 [± 0.093]; P = 0.043). VNS-10 reduced neutrophil influx (15 [± 6]; P = 0.009), while LIS (0.331 [± 0.053]; P = 0.088) was similar. In vagotomized rats, neutrophil influx (52 [± 37]; P = 0.818) and LIS (0.407 [SD ± 0.037]; P = 0.895) in VNS-50-before were similar compared with NOSTIM, as well as in VNS-50-after (neutrophils 30 [± 26]; P = 0.090 and LIS 0.344 [± 0.053]; P = 0.073). In contrast, VNS-50-unilaterally reduced neutrophil influx (26 [± 10]; P = 0.050) and LIS (0.296 [± 0.065]; P = 0.005). Systemic levels of cytokines TNF-α and IL-6 were undetectable in all groups. Pulmonary function was not statistically significantly affected. In conclusion, VNS limited influx of neutrophils in lungs in non-vagotomized rats and may attenuate LIS. Unilateral VNS attenuated lung injury even after ipsilateral vagotomy. This effect was absent for bilateral VNS before and after bilateral vagotomy. It is suggested that the effect of VNS is dependent on (partially) intact vagus nerves and that the level of the vagotomy during esophagectomy may influence postoperative pulmonary outcomes.
Keywords: Esophagectomy; Inflammation; Pulmonary complications; Vagotomy; Vagus nerve; Vagus nerve stimulation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests.
Figures





References
-
- Voeten DM, Busweiler LAD, van der Werf LR, Wijnhoven BPL, Verhoeven RHA, van Sandick JW, et al. Outcomes of esophagogastric cancer surgery during eight years of surgical auditing by the Dutch Upper Gastrointestinal Cancer Audit (DUCA). Ann Surg. 2021;274(5):866–73. 10.1097/SLA.0000000000005116. - PubMed
-
- Muller-Stich BP, Probst P, Nienhuser H, Fazeli S, Senft J, Kalkum E, et al. Meta-analysis of randomized controlled trials and individual patient data comparing minimally invasive with open oesophagectomy for cancer. Br J Surg. 2021;108(9):1026–33. 10.1093/bjs/znab278. - PubMed
-
- Janssen T, Fransen LFC, Heesakkers F, Dolmans-Zwartjes ACP, Moorthy K, Nieuwenhuijzen GAP, et al. Effect of a multimodal prehabilitation program on postoperative recovery and morbidity in patients undergoing a totally minimally invasive esophagectomy. Dis Esophagus. 2021. 10.1093/dote/doab082. - PubMed
-
- Fransen LFC, Janssen T, Aarnoudse M, Nieuwenhuijzen GAP, Luyer MDP. Direct oral feeding after a minimally invasive esophagectomy: a single-center prospective cohort study. Ann Surg. 2022;275(5):919–23. 10.1097/SLA.0000000000004036. - PubMed
-
- Puccetti F, Wijnhoven BPL, Kuppusamy M, Hubka M, Low DE. Impact of standardized clinical pathways on esophagectomy: a systematic review and meta-analysis. Dis Esophagus. 2022;35(2). 10.1093/dote/doab027. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
