

Liraglutide Improves Myocardial Perfusion and Energetics and Exercise Tolerance in Patients With Type 2 Diabetes
- PMID: 39084829
- PMCID: PMC11296502
- DOI: 10.1016/j.jacc.2024.04.064
Liraglutide Improves Myocardial Perfusion and Energetics and Exercise Tolerance in Patients With Type 2 Diabetes
Abstract
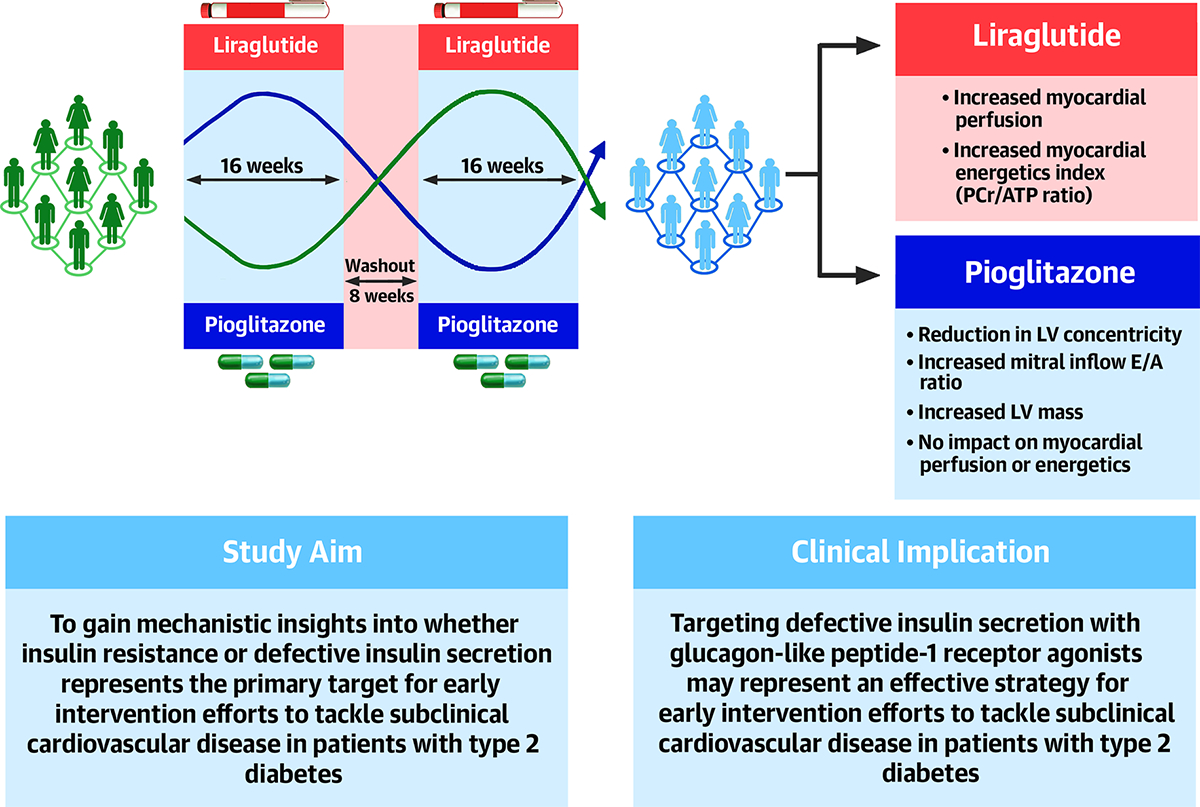
Background: Type 2 diabetes (T2D) is characterized by insulin resistance (IR) and dysregulated insulin secretion. Glucagon-like peptide-1 receptor agonist liraglutide promotes insulin secretion, whereas thiazolidinedione-pioglitazone decreases IR.
Objectives: This study aimed to compare the efficacies of increasing insulin secretion vs decreasing IR strategies for improving myocardial perfusion, energetics, and function in T2D via an open-label randomized crossover trial.
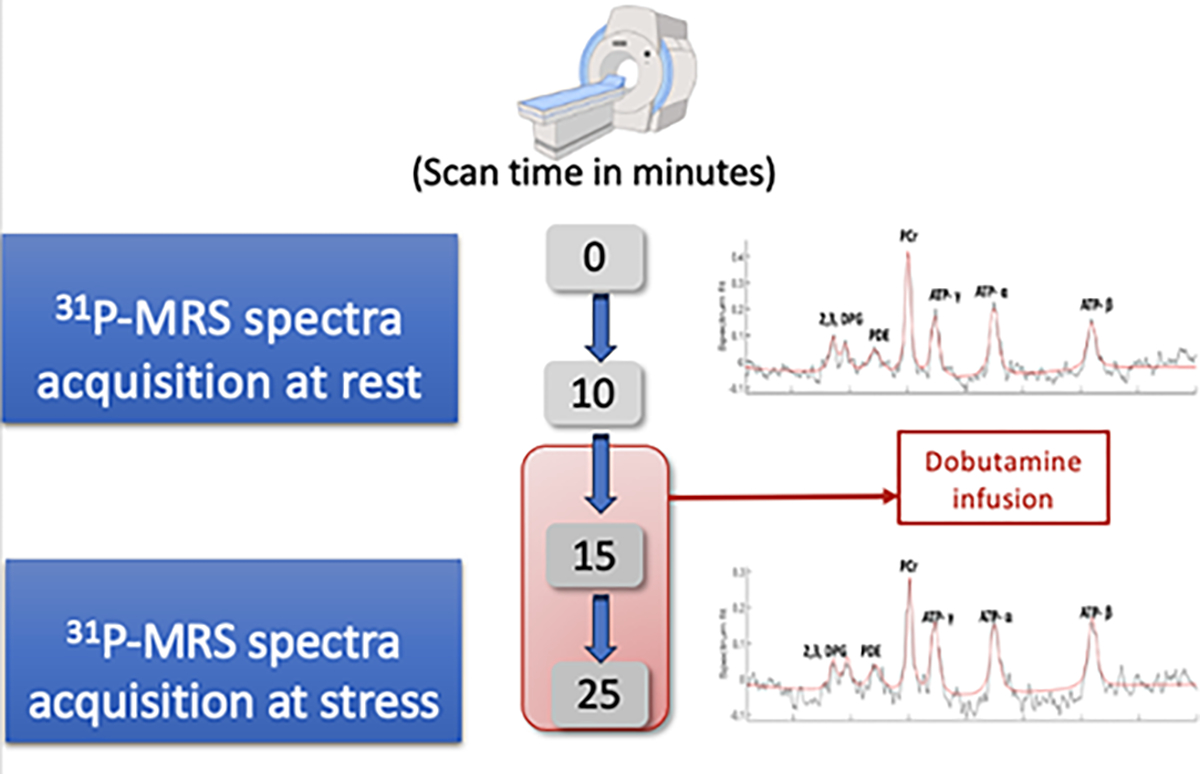
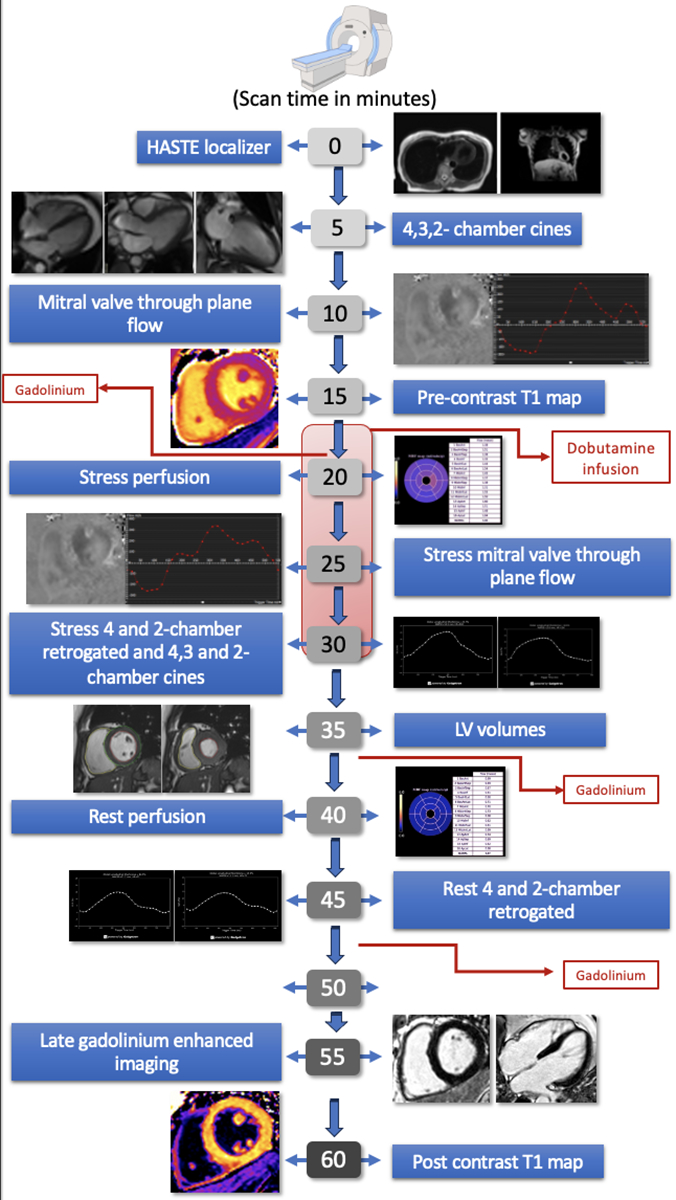
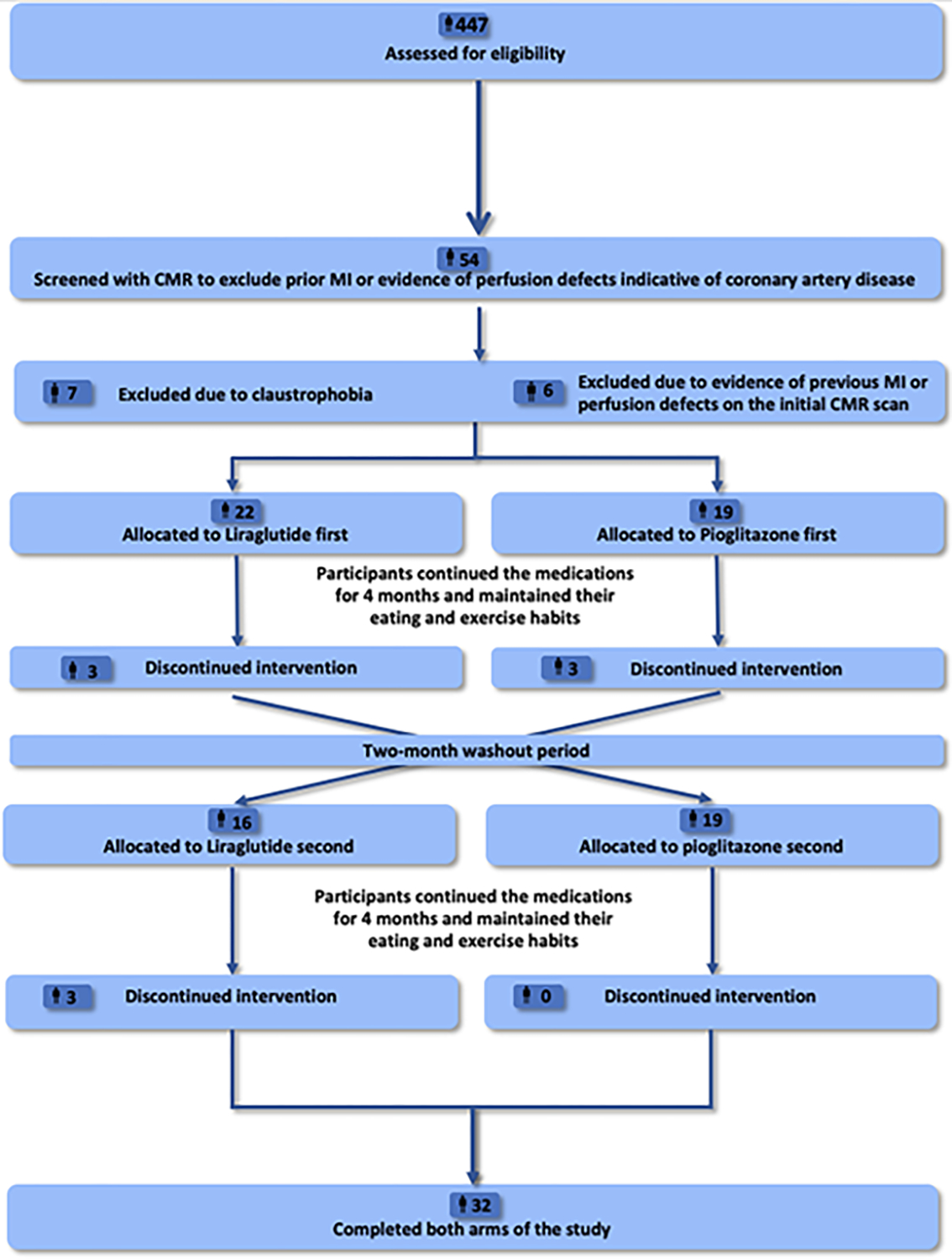
Methods: Forty-one patients with T2D (age 63 years [95% CI: 59-68 years], 27 [66%] male, body mass index 27.8 kg/m2) [95% CI: 26.1-29.5 kg/m2)]) without cardiovascular disease were randomized to liraglutide or pioglitazone for a 16-week treatment followed by an 8-week washout and a further 16-week treatment with the second trial drug. Participants underwent rest and dobutamine stress 31phosphorus magnetic resonance spectroscopy and cardiovascular magnetic resonance for measuring the myocardial energetics index phosphocreatine to adenosine triphosphate ratio, myocardial perfusion (rest, dobutamine stress myocardial blood flow, and myocardial perfusion reserve), left ventricular (LV) volumes, systolic and diastolic function (mitral in-flow E/A ratio), before and after treatment. The 6-minute walk-test was used for functional assessments.
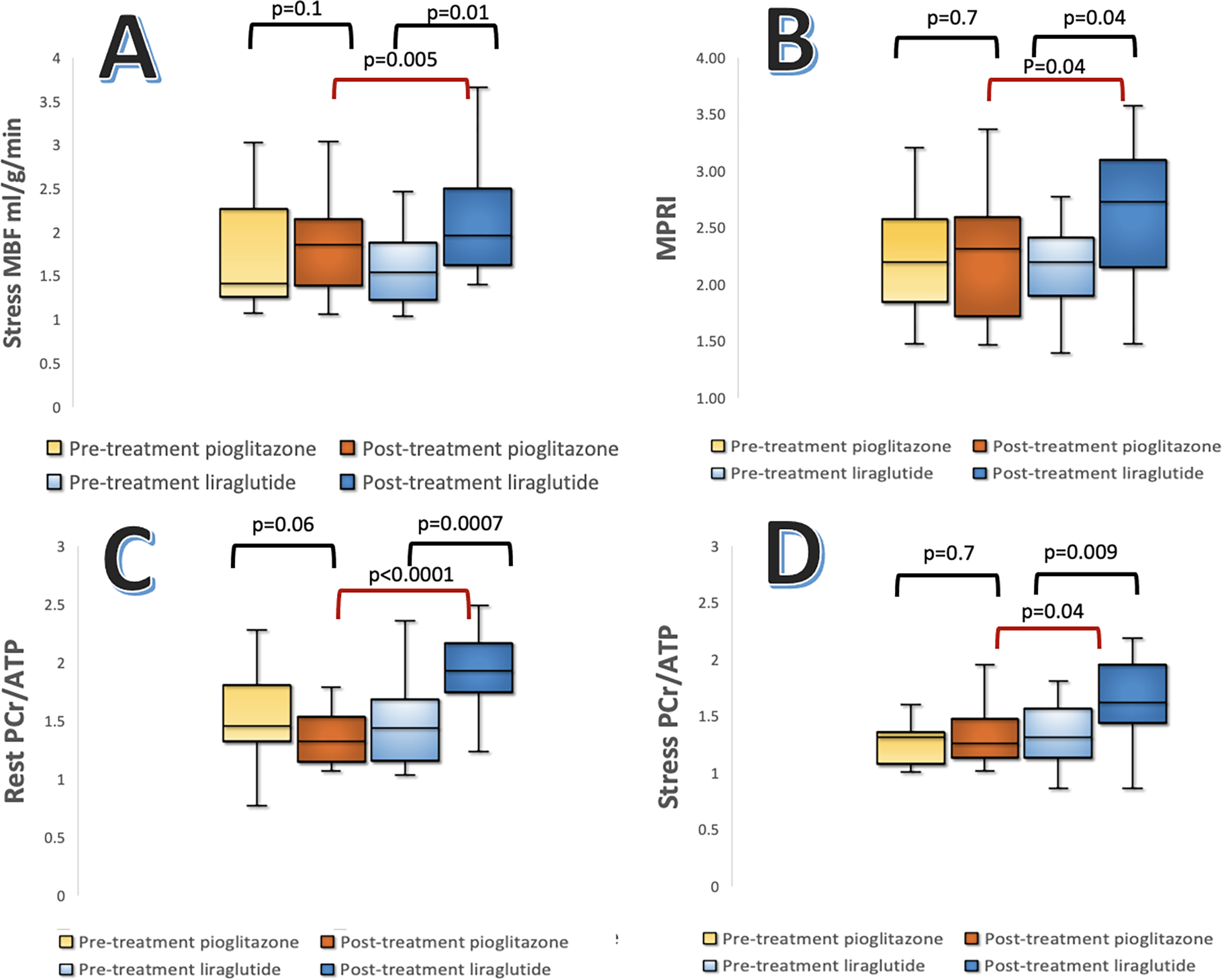
Results: Pioglitazone treatment resulted in significant increases in LV mass (96 g [95% CI: 68-105 g] to 105 g [95% CI: 74-115 g]; P = 0.003) and mitral-inflow E/A ratio (1.04 [95% CI: 0.62-1.21] to 1.34 [95% CI: 0.70-1.54]; P = 0.008), and a significant reduction in LV concentricity index (0.79 mg/mL [95% CI: 0.61-0.85 mg/mL] to 0.73 mg/mL [95% CI: 0.56-0.79 mg/mL]; P = 0.04). Liraglutide treatment increased stress myocardial blood flow (1.62 mL/g/min [95% CI: 1.19-1.75 mL/g/min] to 2.08 mL/g/min [95% CI: 1.57-2.24 mL/g/min]; P = 0.01) and myocardial perfusion reserve (2.40 [95% CI: 1.55-2.68] to 2.90 [95% CI: 1.83-3.18]; P = 0.01). Liraglutide treatment also significantly increased the rest (1.47 [95% CI: 1.17-1.58] to 1.94 [95% CI: 1.52-2.08]; P =0.00002) and stress phosphocreatine to adenosine triphosphate ratio (1.32 [95% CI: 1.05-1.42] to 1.58 [95% CI: 1.19-1.71]; P = 0.004) and 6-minute walk distance (488 m [95% CI: 458-518 m] to 521 m [95% CI: 481-561 m]; P = 0.009).
Conclusions: Liraglutide treatment resulted in improved myocardial perfusion, energetics, and 6-minute walk distance in patients with T2D, whereas pioglitazone showed no effect on these parameters (Lean-DM [Targeting Beta-cell Failure in Lean Patients With Type 2 Diabetes]; NCT04657939).
Keywords: cardiovascular magnetic resonance imaging; glucagon like peptide 1 receptor agonists; liraglutide; magnetic resonance spectroscopy, pioglitazone; type 2 diabetes.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The views expressed are those of the author(s) and not necessarily those of the Wellcome Trust, the NHS, the NIHR, or the Department of Health and Social Care. This independent research has been jointly funded by the Wellcome Trust (grant number: 221690/Z/20/Z) and Diabetes UK (grant number:18/0005870) and has been performed at the National Institute for Health and Care Research (NIHR) Leeds Biomedical Research Centre (BRC) (NIHR203331). Funding for open access charge is from Wellcome Trust (grant number: 221690/Z/20/Z). Dr Chowdhary has received grants from the British Heart Foundation (grant number: FS/CRTF/20/24003). Dr Valkovič has received grants from the Sir Henry Dale Fellowship supported jointly by the Wellcome Trust and the Royal Society (#221805/Z/20/Z), and Slovak Grant Agencies VEGA (#2/0004/23) and APVV (#21-0299). Dr Levelt acknowledges support from the Wellcome Trust Clinical Career Development Fellowship (grant number: 221690/Z/20/Z), Diabetes UK (grant number: UK 18/0005908) and the NIHR Leeds Biomedical Research Centre. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Rawshani A, Rawshani A, Franzén S et al. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. New England Journal of Medicine 2018;379:633–644. - PubMed
-
- Marwick TH, Gimelli A, Plein S et al. Multimodality imaging approach to left ventricular dysfunction in diabetes: an expert consensus document from the European Association of Cardiovascular Imaging. European Heart Journal - Cardiovascular Imaging 2022;23:e62–e84. - PubMed
-
- Sattar N, Lee MMY, Kristensen SL et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. The Lancet Diabetes & Endocrinology 2021;9:653–662. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
