

Colorectal cancer and inflammatory bowel diseases share common salivary proteomic pathways
- PMID: 39085299
- PMCID: PMC11291686
- DOI: 10.1038/s41598-024-68400-z
Colorectal cancer and inflammatory bowel diseases share common salivary proteomic pathways
Abstract
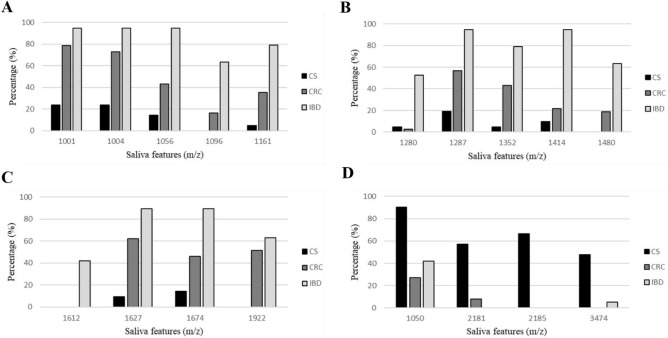
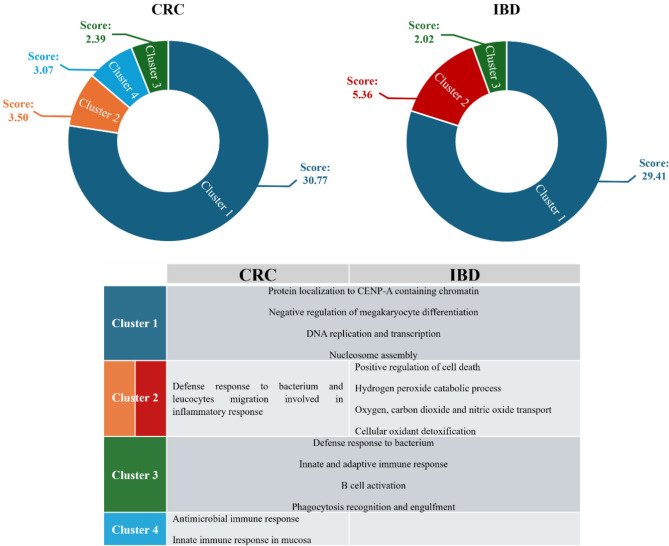
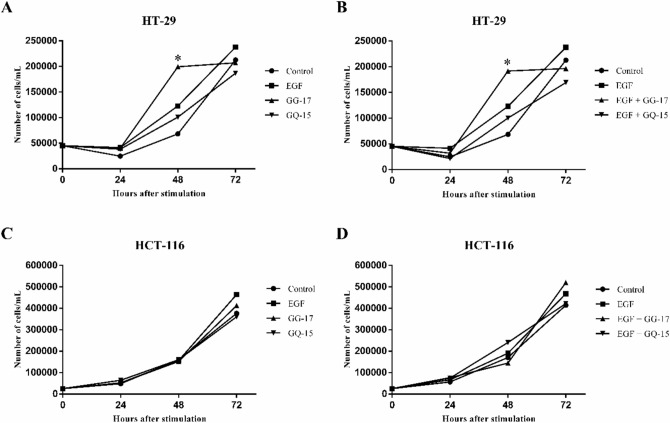
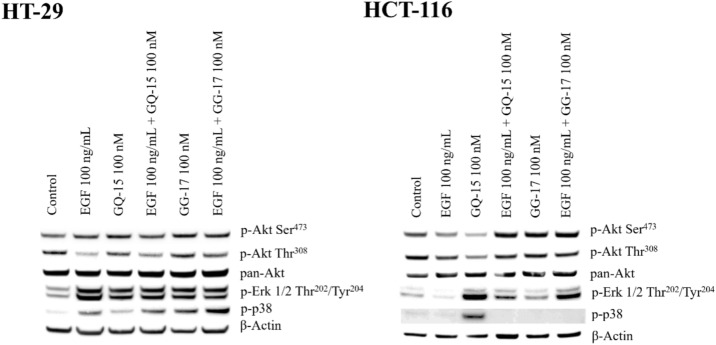
Inflammatory bowels diseases (IBD) are high risk conditions for colorectal cancer (CRC). The discovery of IBD and CRC noninvasive protein/peptide biomarkers using saliva and feces was the aim of this study involving 20 controls, 25 IBD (12 Crohn's Disease-CD), 37 CRC. By untargeted proteomic (LTQ-Orbitrap/MS), a total of 152 proteins were identified in saliva. Absent in controls, 73 proteins were present in both IBD and CRC, being mainly related to cell-adhesion, cadherin-binding and enzyme activity regulation (g-Profiler). Among the remaining 79 proteins, 14 were highly expressed in CD and 11 in CRC. These proteins clustered in DNA replication/expression and innate/adaptive immunity. In stool, endogenous peptides from 30 different proteins were identified, two being salivary and CD-associated: Basic Proline-rich Protein 1 (PRBs) and Acidic Proline-rich Phosphoprotein. Biological effects of the PRBs-related peptides GQ-15 and GG-17 found in CD stool were evaluated using CRC cell lines. These peptides induced cell proliferation and activated Erk1/2, Akt and p38 pathways. In conclusion, the salivary proteome unveiled DNA stability and immunity clusters shared between IBD and CRC. Salivary PRB-derived peptides, enriched in CD stool, stimulate CRC cell proliferation and the pro-oncogenic RAS/RAF/MEK/ERK and PI3K/AKT/mTOR pathways suggesting a potential involvement of PRBs in IBD and cancer pathogenesis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
