

Cranioencephalic functional lymphoid units in glioblastoma
- PMID: 39085419
- PMCID: PMC11485206
- DOI: 10.1038/s41591-024-03152-x
Cranioencephalic functional lymphoid units in glioblastoma
Abstract
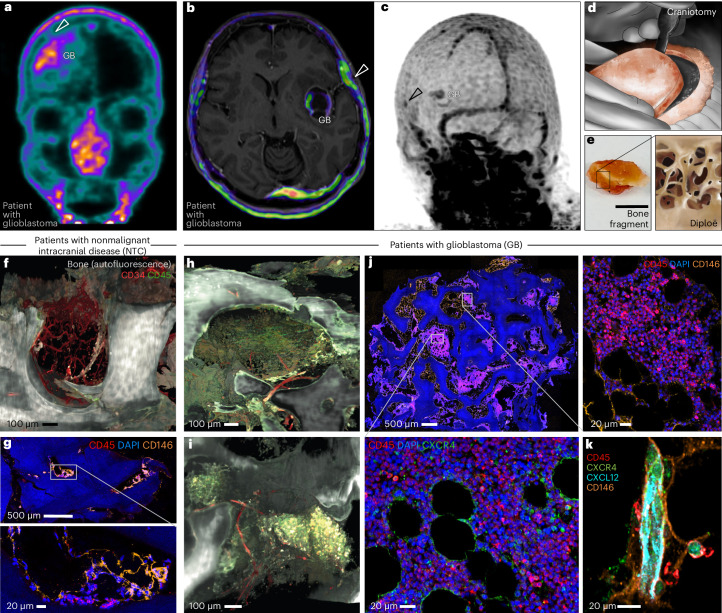
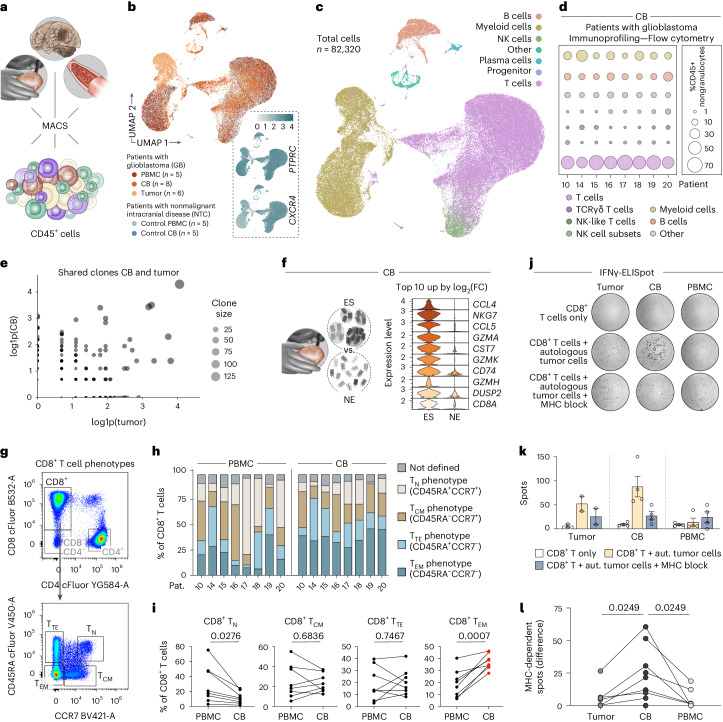
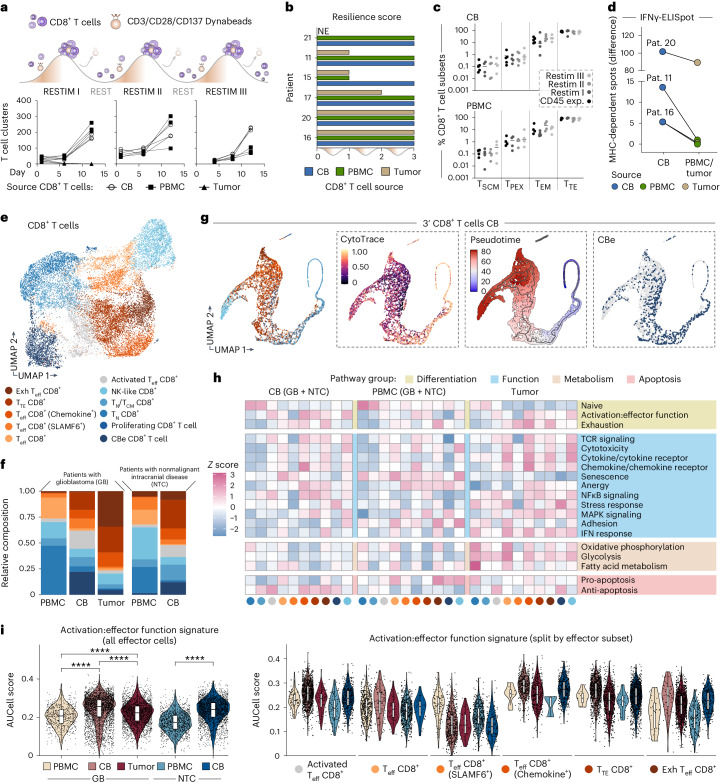
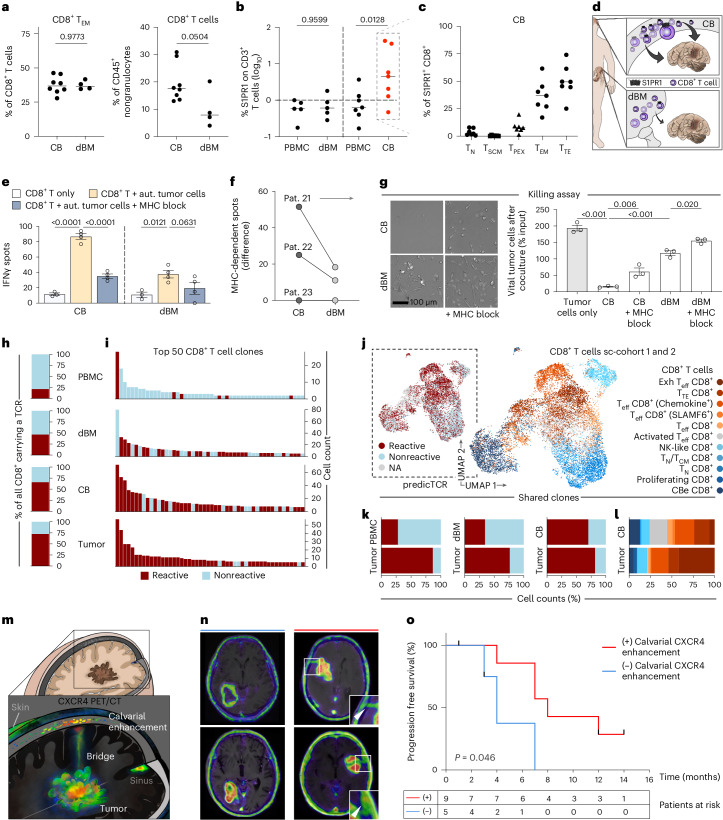
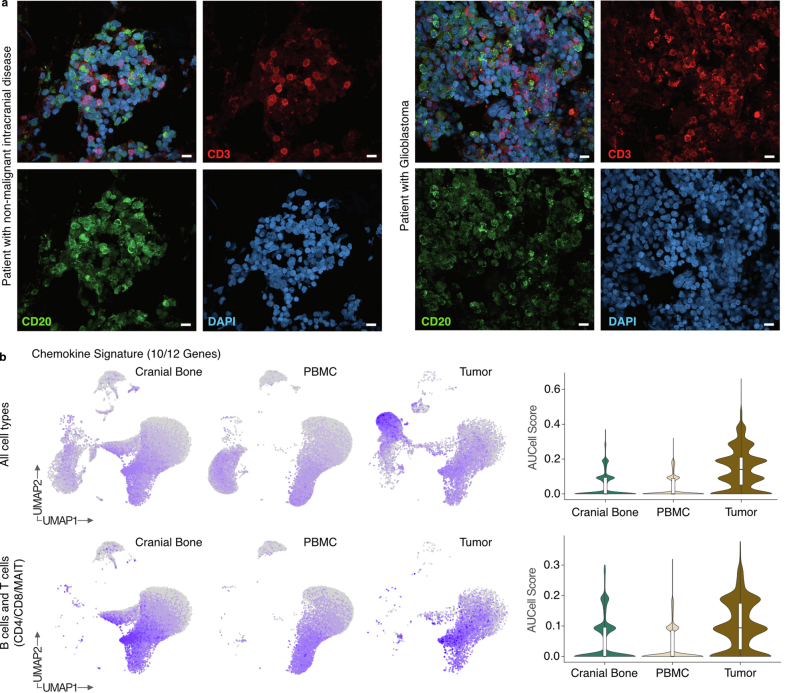
The ecosystem of brain tumors is considered immunosuppressed, but our current knowledge may be incomplete. Here we analyzed clinical cell and tissue specimens derived from patients presenting with glioblastoma or nonmalignant intracranial disease to report that the cranial bone (CB) marrow, in juxtaposition to treatment-naive glioblastoma tumors, harbors active lymphoid populations at the time of initial diagnosis. Clinical and anatomical imaging, single-cell molecular and immune cell profiling and quantification of tumor reactivity identified CD8+ T cell clonotypes in the CB that were also found in the tumor. These were characterized by acute and durable antitumor response rooted in the entire T cell developmental spectrum. In contrast to distal bone marrow, the CB niche proximal to the tumor showed increased frequencies of tumor-reactive CD8+ effector types expressing the lymphoid egress marker S1PR1. In line with this, cranial enhancement of CXCR4 radiolabel may serve as a surrogate marker indicating focal association with improved progression-free survival. The data of this study advocate preservation and further exploitation of these cranioencephalic units for the clinical care of glioblastoma.
© 2024. The Author(s).
Conflict of interest statement
C.D., L.R., D.A.S., F.R., I.C., U.S. and B.S. are inventors on a patent application related to cellular data of this study (EP24160641.7). C.L.T., M.P. and E.W.G. are inventors on a patent application describing the identification of tumor-reactive TCRs (WO 2022/200456). M.D.O. receives consulting fees from Brainlab AG and no support was provided for this study or data presented here. D.A.S. is a cofounder of Round Table Research, focused on oncology and degenerative diseases, with currently unrelated technologies and no support provided for this study or data presented here. R.A.W. has received speaker honoraria from Novartis/AAA and PentixaPharm, reports advisory board work for Novartis/AAA and Bayer and is involved in 68Ga-Pentixafor PET Imaging in PAN Cancer (FORPAN; sponsored and planned by PentixaPharm). A.K.B. has received speaker honoraria from Novartis/AAA and PentixaPharm, is a board member/officer/trustee for PentixaPharm and is involved in 68Ga-Pentixafor PET Imaging in PAN Cancer (FORPAN; sponsored and planned by PentixaPharm). H.C.R. received consulting and lecture fees from AbbVie, AstraZeneca, Roche, Janssen-Cilag, Novartis, Vertex and Merck; has received research funding from Gilead and AstraZeneca; and is a cofounder of CDL Therapeutics GmbH. M.P. and E.W.G. are founders of Tcelltech GmbH. B.S. reports grants from BMWK and DKFZ-Bayer Joint Alliance outside the submitted work. Additionally, B.S. has a patent for peripheral zone tumor cells, methods for their preparation and use issued (EP2324111, AU 2009291203 and USPTO 9,103,819). The other authors declare no competing interests.
Figures









References
MeSH terms
Substances
Grants and funding
- 2019.008.2/Wilhelm Sander-Stiftung (Wilhelm Sander Foundation)
- SCHE656/2-2, proj#405344257/Deutsche Forschungsgemeinschaft (German Research Foundation)
- HE 8145/6-1/5-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- RE 2246/13-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- SFB1399-A01/Deutsche Forschungsgemeinschaft (German Research Foundation)
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
