

Effect of baseline fluid localization on visual acuity and prognosis in type 1 macular neovascularization treated with anti-VEGF
- PMID: 39085593
- PMCID: PMC11543923
- DOI: 10.1038/s41433-024-03256-1
Effect of baseline fluid localization on visual acuity and prognosis in type 1 macular neovascularization treated with anti-VEGF
Abstract
Purpose: To assess the prognostic value of subretinal (SRF) and intraretinal fluid (IRF) localizations in type 1 macular neovascularization (MNV) due to age-related macular degeneration (AMD).
Subjects: Eyes were prospectively treated with anti-vascular epithelial growth factor (anti-VEGF) intravitreal injections (IVT) according to a Pro-Re-Nata (PRN) or Treat and Extend (TAE) regimen during 24 months. A total of 211 eyes with treatment-naïve type 1 MNV secondary to AMD were consecutively included. Eyes were divided between 2 groups according to the fluid localization: presence of SRF alone (SRF group), or presence of IRF associated or not with SRF (IRF ± SRF group).
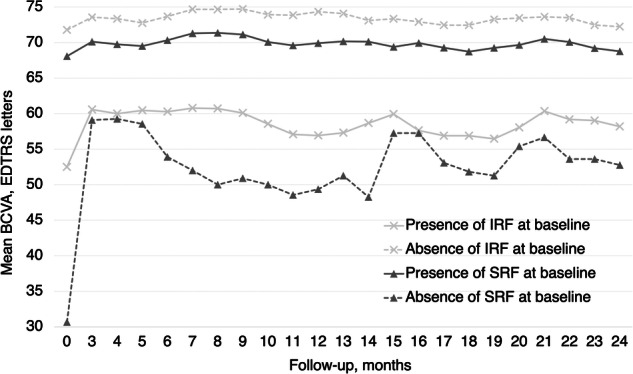
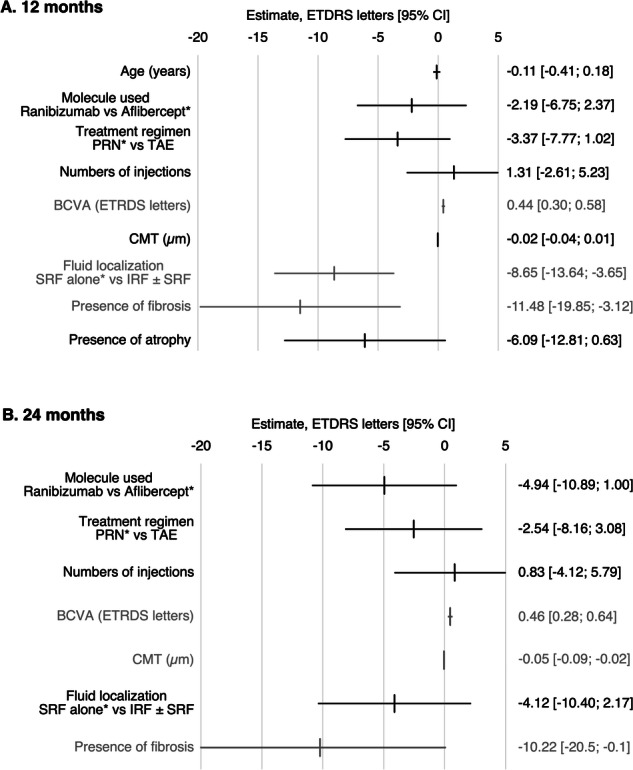
Results: At baseline the mean BCVA was 66.2 letters. SRF was present in 94.8% of eyes, IRF in 30.8%, and both in 25.6%. Data were available for 201 eyes at 12 months, and 157 eyes at 24 months. The presence of IRF at baseline was associated with lower baseline BCVA and significantly lower BCVA at 12 months (p < 0.001) and 24 months (p < 0.001). Eyes with SRF alone displayed better visual outcomes (BCVA at month 12, SRF = 74.3 letters, IRF ± SRF = 56.9 letters). In the presence of baseline IRF, fibrosis (p = 0.03) and atrophy (p < 0.001) were more frequently found at 24 months. In a multivariate model, the presence of baseline IRF was significantly associated with lower BCVA at month 12 but not at month 24.
Conclusion: In type 1 MNV, the presence of baseline IRF was associated with worse visual outcomes compared to SRF alone, and more frequent atrophy and fibrosis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
