

Learning Health System to rapidly improve the implementation of a school physical activity policy
- PMID: 39085972
- PMCID: PMC11292924
- DOI: 10.1186/s43058-024-00619-3
Learning Health System to rapidly improve the implementation of a school physical activity policy
Abstract
Background: Learning Health Systems (LHS) - characterised by cycles of evidence generation and application - are increasingly recognised for their potential to improve public health interventions and optimise health impacts; however there is little evidence of their application in the context of public health practice. Here, we describe how an Australian public health unit applied a LHS approach to successfully improve a model of support for implementation of a school-based physical activity policy.
Methods: This body of work was undertaken in the context of a strong research-practice partnership. Core LHS capabilities included: i) partnerships and stakeholder engagement; ii) workforce development and learning health communities; iii) multi-disciplinary scientific expertise; iv) practice data collection and management system; v) evidence surveillance and synthesis; and vi) governance and organisational processes of decision making. Three cycles of data generation and application were used. Within each cycle, randomised controlled trials conducted in NSW primary schools were used to generate data on the support model's effectiveness for improving schools' implementation of a government physical activity policy, its delivery costs, and process measures such as adoption and acceptability. Each type of data were analysed independently, synthesised, and then presented to a multi-disciplinary team of researchers and practitioners, in consult with stakeholders, leading to collaborative decisions for incremental improvements to the support model.
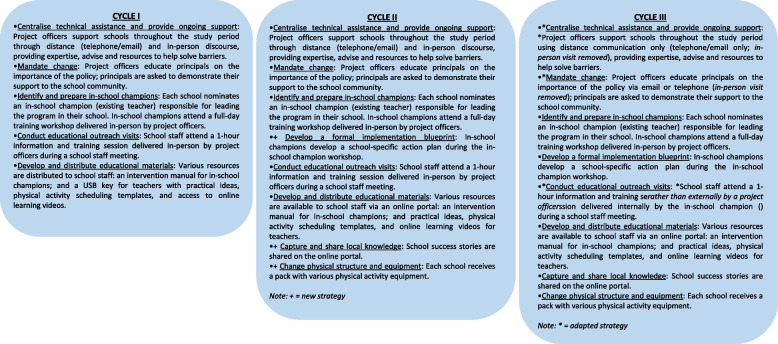
Results: Cycle 1 tested the first version of the support model (composed of five implementation strategies targeting identified barriers of policy implementation) and showed the model's feasibility and efficacy for improving schools' policy implementation. Data-informed changes were made to enhance impact, including the addition of three implementation strategies to address outstanding barriers. Cycle 2 (now, testing a package of eight implementation strategies) established the model's effectiveness and cost-effectiveness for improving school's policy implementation. Data-informed changes were made to reduce delivery costs, specifically adapting the costliest strategies to reduce in-person contact from external support personnel. Cycle 3 showed that the adaptations minimised the relative cost of delivery without adversely impacting on the effect.
Conclusions: Through this process, we identified an effective, cost-effective, acceptable and scalable policy implementation support model for service delivery. This provides important information to inform or support LHS approaches for other agencies seeking to optimise the health impact of evidence-based interventions.
Keywords: Adaptations; Implementation; Learning health systems; Optimisation; Physical activity; Scale-up; School.
© 2024. The Author(s).
Conflict of interest statement
Nicole Nathan and Luke Wolfenden are on the editorial board for Implementation Science Communications.
Figures
References
-
- Sheikh K, Abimbola S; World Health Organization. Learning health systems: pathways to progress: flagship report of the alliance for health policy and systems research. 2021.
-
- Medicine I. Roundtable on value and science-driven health care: the learning health system and its innovation Collaboratives: update report. Washington DC: IOM; 2011.
LinkOut - more resources
Full Text Sources
