

Baseline C-reactive Protein as a Risk Factor for Cryptococcal Meningitis and Death in HIV-associated Cryptococcal Antigenemia With CrAg Titer as an Effect Modifier
- PMID: 39086467
- PMCID: PMC11288378
- DOI: 10.1093/ofid/ofae392
Baseline C-reactive Protein as a Risk Factor for Cryptococcal Meningitis and Death in HIV-associated Cryptococcal Antigenemia With CrAg Titer as an Effect Modifier
Abstract
Background: Persons with HIV and cryptococcal antigenemia are at high risk of progression to cryptococcal meningitis or death. Baseline cryptococcal antigen (CrAg) plasma titer ≥1:160 is a known risk factor for poor outcomes, but other risk factors are unknown. In HIV-associated cryptococcal meningitis, baseline serum C-reactive protein (CRP) concentrations are positively associated with increased mortality. We hypothesized that CRP might also be associated with meningitis or death in persons with cryptococcal antigenemia.
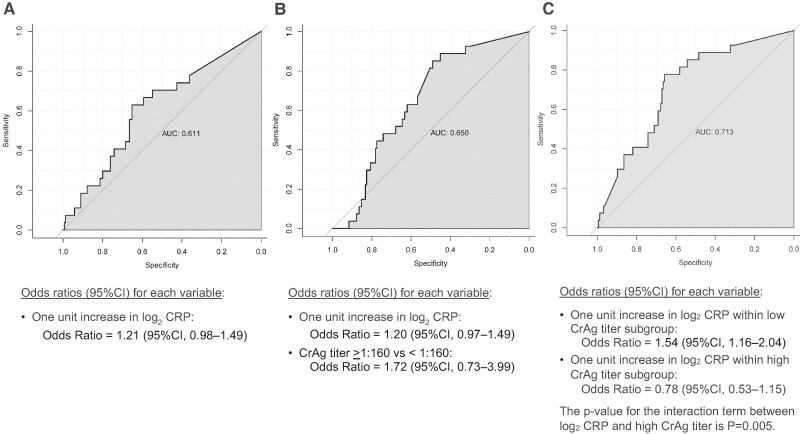
Methods: We measured plasma CrAg titers and CRP concentrations on cryopreserved serum from prospectively enrolled persons with HIV and cryptococcal antigenemia. Using time-to-event analyses, we compared 24-week meningitis-free survival in persons with normal CRP (<8 mg/L) and elevated CRP (≥8 mg/L). Logistic regression was used to assess how CRP concentration and CrAg titer might interact as covariates.
Results: Of the 94 persons with elevated CRP, 19 (20.2%) developed meningitis or death, whereas of the 88 persons with normal CRP, 8 (9.1%) developed meningitis or death (P = .035). Persons with CrAg titer <1:160 and normal CRP had an ∼5% (3/61) event rate, whereas those with CrAg titer <1:160 but elevated CRP had an ∼20% (12/59) event rate. Importantly, we identified a statistically significant interaction effect between CrAg titer and CRP groups, in which elevated CRP increased risk in the low CrAg titer group (odds ratio, 1.54; 95% confidence interval, 1.16-2.04), but this effect was not present in high CrAg titer group (odds ratio, 0.78; 95% confidence interval, .53-1.15).
Conclusions: Our findings demonstrate that CrAg titer may modify the direction of effect of CRP with meningitis-free survival; future studies should account for this interaction.
Keywords: HIV; c-reactive protein; cryptococcal antigen titers; cryptococcal antigenemia; cryptococcal meningitis.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts.
Figures


References
-
- Castelnuovo B, Manabe YC, Kiragga A, Kamya M, Easterbrook P, Kambugu A. Cause-specific mortality and the contribution of immune reconstitution inflammatory syndrome in the first 3 years after antiretroviral therapy initiation in an urban African cohort. Clin Infect Dis 2009; 49:965–72. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
