

Definition of a microbial signature as a predictor of endoscopic post-surgical recurrence in patients with Crohn's disease
- PMID: 39086694
- PMCID: PMC11285546
- DOI: 10.3389/fmmed.2023.1046414
Definition of a microbial signature as a predictor of endoscopic post-surgical recurrence in patients with Crohn's disease
Abstract
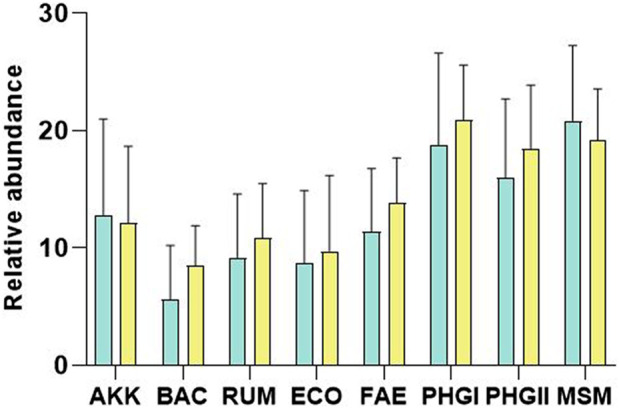
Background and aims: Although there are several effective drugs for the treatment of Crohn's disease (CD), almost 70% of patients will require surgical resection during their lifetime. This procedure is not always curative, as endoscopic recurrence occurs in 65%-90% of patients in the first year after surgery. The aetiology of the recurrence is unknown; however, several studies have shown how the resident microbiota is modified after surgery. The aim of this study was to evaluate samples from patients with Crohn's disease before and after an intestinal resection to determine whether there were differences in the abundance of different microbial markers, which may predict endoscopic recurrence at baseline. Methods: In this observational study, a stool sample was obtained from 25 patients with Crohn's disease before undergoing surgery, recruited at three Catalan hospitals. From each sample, DNA was purified and the relative abundance of nine microbial markers was quantified using qPCR. Results: An algorithm composed of four microbial markers (E. coli, F. prausnitzii phylogroup I, Bacteroidetes, and Eubacteria) showed a sensitivity and specificity of 90.91% and 85.71%, respectively, and a positive and negative predictive value of 83.33% and 92.31%, respectively. Conclusion: A microbial signature to determine patients who will have post-surgical recurrence was identified. This tool might be very useful in daily clinical practice, allowing the scheduling of personalized therapy and enabling preventive treatment only in patients who really require it.
Keywords: Crohn’s disease; endoscopic recurrence; gut microbiota; precision medicine; surgical resection.
Copyright © 2023 Oliver, Camps, Julià-Bergkvist, Amoedo, Ramió-Pujol, Malagón, Bahí, Torres, Domènech, Guardiola, Serra-Pagès, Garcia-Gil and Aldeguer.
Conflict of interest statement
GoodGut S.L.U shares the patent PCT/EP 2016/069188 method for the quantification of Faecalibacterium prausnitzii phylogroup I and/or phylogroup II and the use thereof as biomarkers, referenced in this study.
Figures


References
-
- Ayling R. M., Kok K. (2018). Fecal Calprotectin, 87. Amsterdam, Netherlands: Elsevier.
-
- Boschetti G., Laidet M., Moussata D., Stefanescu C., Roblin X., Phelip G., et al. (2015). Levels of fecal calprotectin are associated with the severity of postoperative endoscopic recurrence in asymptomatic patients with Crohn’s disease. Am. J. Gastroenterology 110 (6), 865–872. 10.1038/ajg.2015.30 - DOI - PubMed
LinkOut - more resources
Full Text Sources