

Case Report: Surgical challenges and insights in a child with a blunt left diaphragmatic and pericardial rupture and heart subluxation
- PMID: 39086919
- PMCID: PMC11288843
- DOI: 10.3389/fsurg.2024.1369255
Case Report: Surgical challenges and insights in a child with a blunt left diaphragmatic and pericardial rupture and heart subluxation
Abstract
Introduction: Blunt diaphragmatic rupture (BTDR) is a rare condition that can occur in children following high-energy blunt thoracoabdominal trauma. In less than 1% of the cases, pericardial rupture can coexist with a BTDR. A coexistence of BTDR and pericardial rupture can result in displacement of the heart and is associated with high mortality. Clinical presentation is non-specific and requires a high index of suspicion for early management.
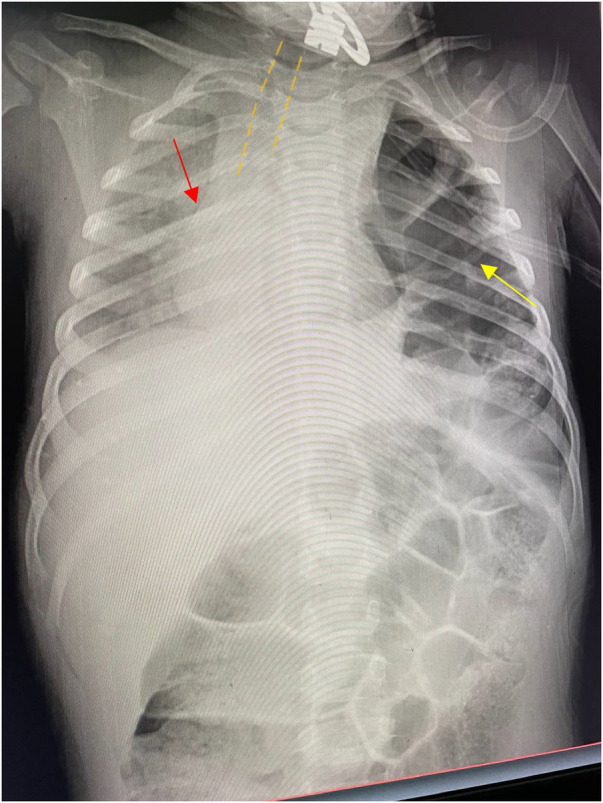
Case presentation: A 4-year-old child presented to the emergency unit of our hospital following high-energy trauma with severe respiratory distress. Initially, a left-side chest tube was inserted, but it resulted in no clinical improvement. A chest x-ray showed a collapse of the left lung with a herniation of bowel loops into the left hemithorax. An exploratory laparotomy was done, which revealed a 10 cm × 4 cm defect in the left hemidiaphragm with a medial extension involving the pericardium. The fundus of the stomach and left lobe of the liver were displaced into the pericardial space, pushing the cardiac apex posteriorly to the right side. Concomitantly, the transverse colon and small bowel were displaced into the left pleural space. After the reduction of the herniated abdominal viscera back into the peritoneal cavity, the pericardial sac was repaired by employing an interrupted resorbable suture, while the diaphragmatic defect was repaired by using a horizontal mattress. No other injuries were identified and the abdomen was closed in layers.
Conclusion: BTDR with pericardial rupture is an elusive condition with a high mortality rate that necessitates a high index of clinical suspicion. Early surgical repair of the defect with a reduction of herniated organs can reduce morbidity and mortality.
Keywords: blunt trauma; diaphragmatic rupture; heart subluxation; pediatric trauma; pericardial tear.
© 2024 Kassie, Ayana, Abebe and Abebe.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Post-traumatic diaphragmatic rupture with pericardial denudation: A case report.Int J Surg Case Rep. 2021 Jun;83:105970. doi: 10.1016/j.ijscr.2021.105970. Epub 2021 May 15. Int J Surg Case Rep. 2021. PMID: 34029846 Free PMC article.
-
Minimally invasive surgery for concomitant pericardial and diaphragmatic rupture after blunt trauma: a case report.J Trauma Inj. 2025 Mar;38(1):51-55. doi: 10.20408/jti.2024.0045. Epub 2024 Dec 16. J Trauma Inj. 2025. PMID: 40175079 Free PMC article.
-
Traumatic Diaphragmatic Rupture With Pericardial Tear and Transdiaphragmatic Herniation of the Stomach.Cureus. 2022 Sep 22;14(9):e29473. doi: 10.7759/cureus.29473. eCollection 2022 Sep. Cureus. 2022. PMID: 36299973 Free PMC article.
-
Traumatic Diaphragmatic Rupture with Transthoracic Organ Herniation: A Case Report and Review of Literature.Am J Case Rep. 2020 Jan 3;21:e919442. doi: 10.12659/AJCR.919442. Am J Case Rep. 2020. PMID: 31896740 Free PMC article. Review.
-
Emergency surgery due to diaphragmatic hernia: case series and review.World J Emerg Surg. 2017 May 18;12:23. doi: 10.1186/s13017-017-0134-5. eCollection 2017. World J Emerg Surg. 2017. PMID: 28529538 Free PMC article. Review.
References
-
- Feliciano DV, Mattox KL, Moore EE. Trauma. 9th ed. New York, NY: McGraw Hill; (2020).
-
- Burhamah W, Matcovici M, Hardy A, Awadalla S. Traumatic diaphragmatic rupture in children. J Pediatr Surg Case Rep. (2020) 61:101619. 10.1016/j.epsc.2020.101619 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous