

Pancreatic pseudocyst: The past, the present, and the future
- PMID: 39087130
- PMCID: PMC11287700
- DOI: 10.4240/wjgs.v16.i7.1986
Pancreatic pseudocyst: The past, the present, and the future
Abstract
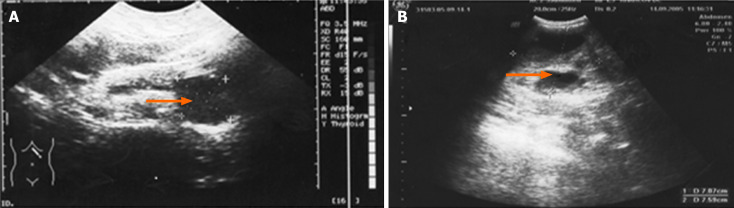
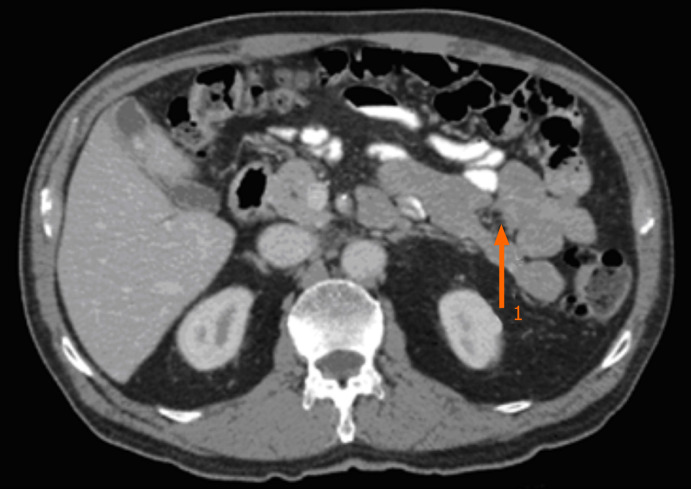
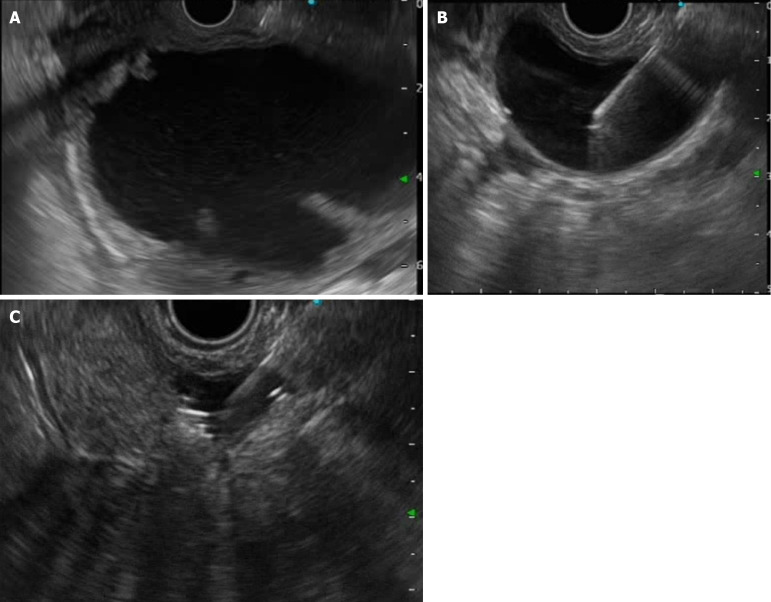
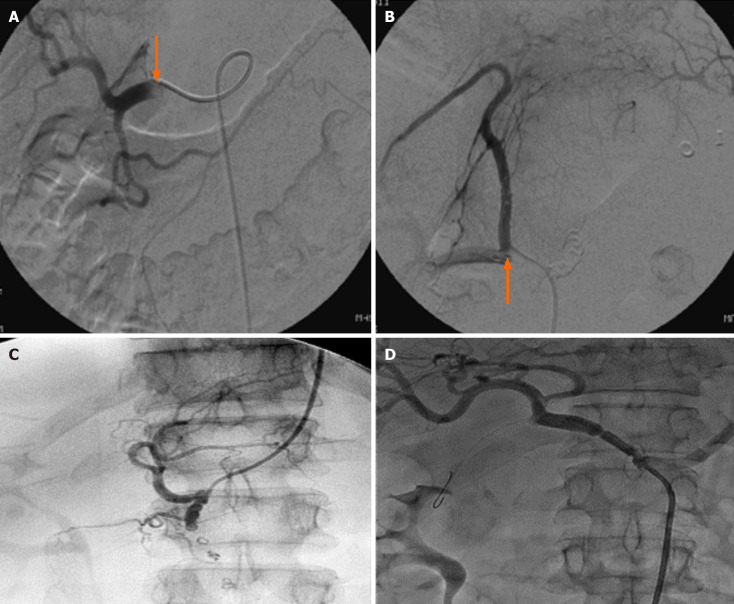
A pancreatic pseudocyst is defined as an encapsulated fluid collection with a well-defined inflammatory wall with minimal or no necrosis. The diagnosis cannot be made prior to 4 wk after the onset of pancreatitis. The clinical presentation is often nonspecific, with abdominal pain being the most common symptom. If a diagnosis is suspected, contrast-enhanced computed tomography and/or magnetic resonance imaging are performed to confirm the diagnosis and assess the characteristics of the pseudocyst. Endoscopic ultrasound with cyst fluid analysis can be performed in cases of diagnostic uncertainty. Pseudocyst of the pancreas can lead to complications such as hemorrhage, infection, and rupture. The management of pancreatic pseudocysts depends on the presence of symptoms and the development of complications, such as biliary or gastric outlet obstruction. Management options include endoscopic or surgical drainage. The aim of this review was to summarize the current literature on pancreatic pseudocysts and discuss the evolution of the definitions, diagnosis, and management of this condition.
Keywords: Cystic pancreatic lesions; Endoscopic ultrasound; Pancreatic fluid collection; Pancreatic pseudocyst; Pancreatitis.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
References
-
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. - PubMed
-
- Gumaste VV, Aron J. Pseudocyst management: endoscopic drainage and other emerging techniques. J Clin Gastroenterol. 2010;44:326–331. - PubMed
-
- Grace PA, Williamson RC. Modern management of pancreatic pseudocysts. Br J Surg. 1993;80:573–581. - PubMed
-
- Sankaran S, Walt AJ. The natural and unnatural history of pancreatic pseudocysts. Br J Surg. 1975;62:37–44. - PubMed
-
- Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg. 1993;128:586–590. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
