

Association Between Achievement of Clinical Disease Control and Improvement in Patient-Reported Outcomes and Quality of Life in Patients With Psoriatic Arthritis in the Phase 3 SELECT-PsA 1 and 2 Randomized Controlled Trials
- PMID: 39087872
- PMCID: PMC11557994
- DOI: 10.1002/acr2.11714
Association Between Achievement of Clinical Disease Control and Improvement in Patient-Reported Outcomes and Quality of Life in Patients With Psoriatic Arthritis in the Phase 3 SELECT-PsA 1 and 2 Randomized Controlled Trials
Abstract
Objective: We explored the relationship between achievement of clinical disease control and improvements in and normative values for patient-reported outcomes (PROs), including quality of life (QoL) measures, in patients with psoriatic arthritis (PsA).
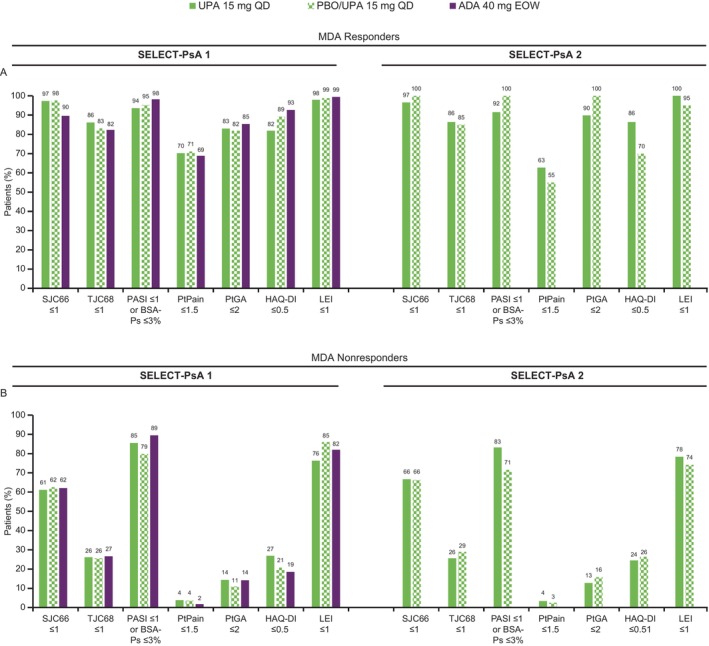
Methods: This was a post hoc analysis of 104-week data from the SELECT-PsA 1 and 2 trials in adults with PsA and inadequate response to one or more conventional synthetic (SELECT-PsA 1) or biologic (SELECT-PsA 2) disease-modifying antirheumatic drug. Patients were initially randomized to upadacitinib 15 mg once daily (QD) to placebo switched to upadacitinib 15 mg QD at week 24 or to adalimumab 40 mg every other week (SELECT-PsA 1 only), and data were pooled across treatments and analyzed. We evaluated several clinical disease control measures (minimal disease activity [MDA]; very low disease activity [VLDA]; and low disease activity [LDA] and/or remission by Disease Activity in Psoriatic Arthritis [DAPSA], Psoriatic Arthritis Disease Activity Score [PASDAS], and Routine Assessment of Patient Index Data 3 [RAPID3]) and examined their associations with improvements and normative values for various PROs.
Results: A total of 1,069 and 317 patients were analyzed for SELECT-PsA 1 and 2, respectively. In both studies, responders (patients who achieved MDA or VLDA, and DAPSA, PASDAS, and RAPID3 LDA or remission) at week 104 achieved more marked changes from baseline, and more responders achieved normative values in PROs compared with nonresponders (most nominal P < 0.0001). Furthermore, numerically larger proportions of responders achieved minimal clinically important differences across PROs compared with nonresponders in both studies. In addition, patients who achieved MDA or VLDA were more likely to achieve DAPSA, PASDAS, and RAPID3 LDA or remission (all nominal P < 0.0001) for upadacitinib 15 mg QD and when treatment arms were pooled.
Conclusion: Patients with PsA who achieve clinical disease control are more likely to achieve improvements and normative values in PROs and QoL measures, which reinforces disease control as a treatment target.
© 2024 AbbVie and The Author(s). ACR Open Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures




References
-
- Coates LC, Fransen J, Helliwell PS. Defining minimal disease activity in psoriatic arthritis: a proposed objective target for treatment. Ann Rheum Dis 2010;69(1):48–53. - PubMed
-
- Coates LC, Helliwell PS. Defining low disease activity states in psoriatic arthritis using novel composite disease instruments. J Rheumatol 2016;43(2):371–375. - PubMed
-
- Schoels M, Aletaha D, Funovits J, et al. Application of the DAREA/DAPSA score for assessment of disease activity in psoriatic arthritis. Ann Rheum Dis 2010;69(8):1441–1447. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
