

Prolonged vs shorter awake prone positioning for COVID-19 patients with acute respiratory failure: a multicenter, randomised controlled trial
- PMID: 39088076
- PMCID: PMC11306533
- DOI: 10.1007/s00134-024-07545-x
Prolonged vs shorter awake prone positioning for COVID-19 patients with acute respiratory failure: a multicenter, randomised controlled trial
Abstract
Purpose: Awake prone positioning has been reported to reduce endotracheal intubation in patients with coronavirus disease 2019 (COVID-19)-related acute hypoxemic respiratory failure (AHRF). However, it is still unclear whether using the awake prone positioning for longer periods can further improve outcomes.
Methods: In this randomized, open-label clinical trial conducted at 12 hospitals in China, non-intubated patients with COVID-19-related AHRF were randomly assigned to prolonged awake prone positioning (target > 12 h daily for 7 days) or standard care with a shorter period of awake prone positioning. The primary outcome was endotracheal intubation within 28 days after randomization. The key secondary outcomes included mortality and adverse events.
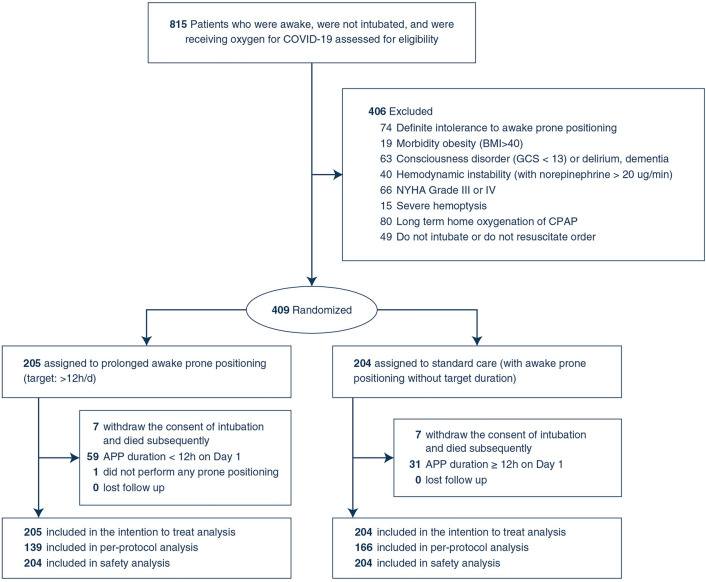
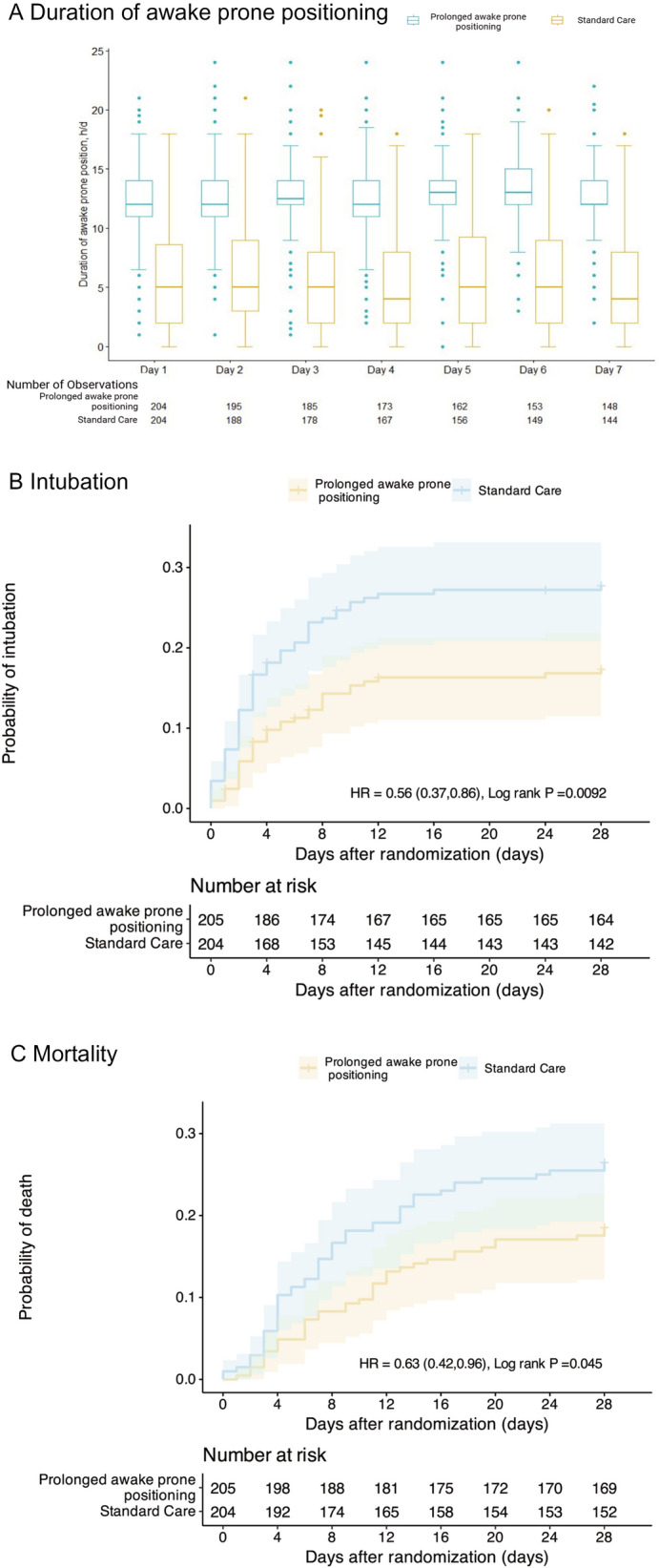
Results: In total, 409 patients were enrolled and randomly assigned to prolonged awake prone positioning (n = 205) or standard care (n = 204). In the first 7 days after randomization, the median duration of prone positioning was 12 h/d (interquartile range [IQR] 12-14 h/d) in the prolonged awake prone positioning group vs. 5 h/d (IQR 2-8 h/d) in the standard care group. In the intention-to-treat analysis, intubation occurred in 35 (17%) patients assigned to prolonged awake prone positioning and in 56 (27%) patients assigned to standard care (relative risk 0.62 [95% confidence interval (CI) 0.42-0.9]). The hazard ratio (HR) for intubation was 0.56 (0.37-0.86), and for mortality was 0.63 (0.42-0.96) for prolonged awake prone positioning versus standard care, within 28 days. The incidence of pre-specified adverse events was low and similar in both groups.
Conclusion: Prolonged awake prone positioning of patients with COVID-19-related AHRF reduces the intubation rate without significant harm. These results support prolonged awake prone positioning of patients with COVID-19-related AHRF.
Trial registration: ClinicalTrials.gov NCT05677984.
Keywords: COVID-19-related acute respiratory failure; Intubation; Mortality; Prolonged awake prone positioning.
© 2024. The Author(s).
Conflict of interest statement
All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work. All authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
- 2022YFC2504405/National Key Research and Development Program of China
- 82341032/National Natural Science Foundation of China
- 81930058/National Natural Science Foundation of China
- 82270083/National Natural Science Foundation of China
- LGY2022025/Project of High-level Teachers in Beijing Municipal Universities in the Period of 13th Five-year Plan
LinkOut - more resources
Full Text Sources
Medical
