

Loss to follow-up and its predictors among children living with HIV on antiretroviral therapy, southern Oromia, Ethiopia: a 5-year retrospective cohort study
- PMID: 39089715
- PMCID: PMC11293378
- DOI: 10.1136/bmjopen-2023-078370
Loss to follow-up and its predictors among children living with HIV on antiretroviral therapy, southern Oromia, Ethiopia: a 5-year retrospective cohort study
Abstract
Background: Loss to follow-up (LTFU) among paediatric patients living with HIV presents a significant challenge to the global scale-up of life-saving antiretroviral therapy (ART).
Objectives: This study aims to estimate LTFU incidence and its determinants among children with HIV on ART in Shashemene town public health institutions, Oromia, Ethiopia.
Design: A retrospective cohort study from 1 January 2015 to 30 December 2020.
Setting: This study was conducted in Shashemene town, Oromia, Ethiopia.
Participants: Medical records of 269 children receiving ART at health facilities in Shashemene town were included.
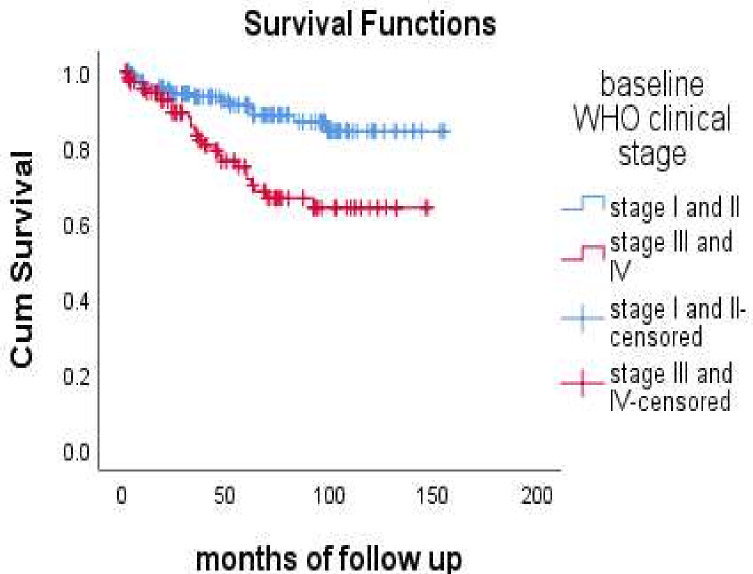
Methods: Data from patients' medical records were collected using a standardised checklist. EpiData V.3.1 was employed for data entry, while Statistical Package for the Social Sciences (SPSS) V.25 facilitated analysis. The Kaplan-Meier survival curve was used for estimation of survival time. To measure association, adjusted HRs (AHRs) with 95% CIs were calculated. Both bivariable and multivariable Cox proportional hazards regression models were employed to identify predictors of LTFU.
Results: Of the 269 children living with HIV included in the final analysis, 43 (16%) were lost to follow-up. The overall incidence rate of LTFU was 3.3 (95% CI 2.4 to 4.4) per 100 child-years of observation. Age less than 5 years (AHR 0.03, 95% CI 0.00 to 0.36), non-orphan status of the child (AHR 0.13, 95% CI 0.05 to 0.34), < 30 min distance to health facility (AHR 0.24, 95% CI 0.08 to 0.73), disclosed HIV status (AHR 0. 32, 95% CI 0.13 to 0.80), history of opportunistic infection (AHR 3.54, 95% CI 1.15 to 10.87) and low CD4 count (AHR 5.17, 95% CI 2.08 to 12.85) were significant predictors of LTFU.
Conclusion: The incidence rate of LTFU was lower compared with other studies in Ethiopia. This result indicated that age less than 5 years, non-orphans, low CD4, disclosed HIV status and distance from health facility were predictors of LTFU.
Keywords: Epidemiology; HIV & AIDS; PUBLIC HEALTH.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- UNAIDS . AIDS info website; 2019. [-Jul-2020]. UNAIDS. 2020 HIV and AIDS estimates ethiopia, UNAIDS country factsheets – 2020 fact sheet.http://aidsinfo.unaids.org/ Available. Accessed.
-
- UNAIDS Global AIDS update 2019. 2019
-
- WHO . Switzerland: Glion; 2015. WHO working group on HIV incidence assays: estimating HIV incidence using HIV case surveillance: meeting report; pp. 10–1.
-
- FMOH E. National Consolidated Guidelines for Comprehensive HIV Prevention, Care and Treatment. 2018.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials