

Tregs delivered post-myocardial infarction adopt an injury-specific phenotype promoting cardiac repair via macrophages in mice
- PMID: 39090108
- PMCID: PMC11294480
- DOI: 10.1038/s41467-024-50806-y
Tregs delivered post-myocardial infarction adopt an injury-specific phenotype promoting cardiac repair via macrophages in mice
Abstract
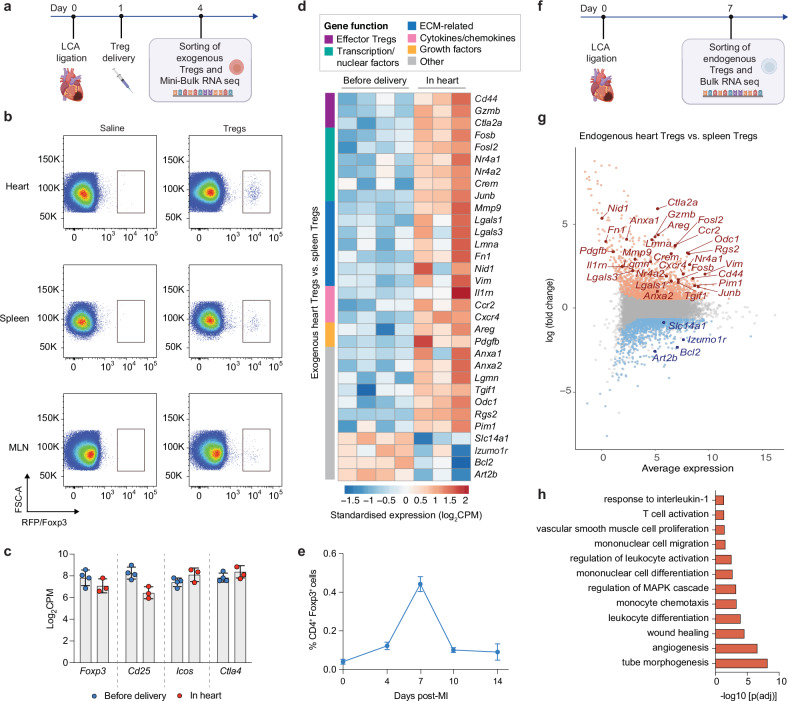
Regulatory T cells (Tregs) are key immune regulators that have shown promise in enhancing cardiac repair post-MI, although the mechanisms remain elusive. Here, we show that rapidly increasing Treg number in the circulation post-MI via systemic administration of exogenous Tregs improves cardiac function in male mice, by limiting cardiomyocyte death and reducing fibrosis. Mechanistically, exogenous Tregs quickly home to the infarcted heart and adopt an injury-specific transcriptome that mediates repair by modulating monocytes/macrophages. Specially, Tregs lead to a reduction in pro-inflammatory Ly6CHi CCR2+ monocytes/macrophages accompanied by a rapid shift of macrophages towards a pro-repair phenotype. Additionally, exogenous Treg-derived factors, including nidogen-1 and IL-10, along with a decrease in cardiac CD8+ T cell number, mediate the reduction of the pro-inflammatory monocyte/macrophage subset in the heart. Supporting the pivotal role of IL-10, exogenous Tregs knocked out for IL-10 lose their pro-repair capabilities. Together, this study highlights the beneficial use of a Treg-based therapeutic approach for cardiac repair with important mechanistic insights that could facilitate the development of novel immunotherapies for MI.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
