

Colorectal cancer risk stratification using a polygenic risk score in symptomatic primary care patients-a UK Biobank retrospective cohort study
- PMID: 39090236
- PMCID: PMC11577060
- DOI: 10.1038/s41431-024-01654-3
Colorectal cancer risk stratification using a polygenic risk score in symptomatic primary care patients-a UK Biobank retrospective cohort study
Abstract
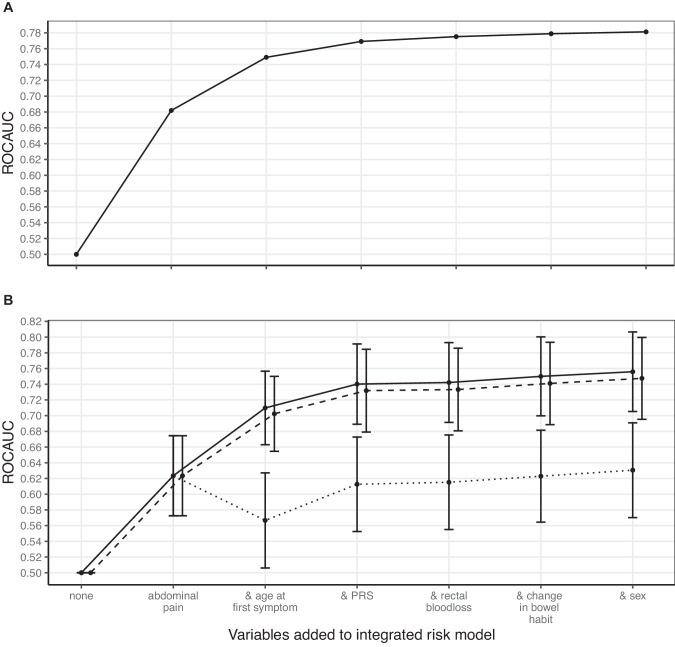
Colorectal cancer (CRC) is a leading cause of cancer mortality worldwide. Accurate cancer risk assessment approaches could increase rates of early CRC diagnosis, improve health outcomes for patients and reduce pressure on diagnostic services. The faecal immunochemical test (FIT) for blood in stool is widely used in primary care to identify symptomatic patients with likely CRC. However, there is a 6-16% noncompliance rate with FIT in clinic and ~90% of patients over the symptomatic 10 µg/g test threshold do not have CRC. A polygenic risk score (PRS) quantifies an individual's genetic risk of a condition based on many common variants. Existing PRS for CRC have so far been used to stratify asymptomatic populations. We conducted a retrospective cohort study of 50,387 UK Biobank participants with a CRC symptom in their primary care record at age 40+. A PRS based on 201 variants, 5 genetic principal components and 22 other risk factors and markers for CRC were assessed for association with CRC diagnosis within 2 years of first symptom presentation using logistic regression. Associated variables were included in an integrated risk model and trained in 80% of the cohort to predict CRC diagnosis within 2 years. An integrated risk model combining PRS, age, sex, and patient-reported symptoms was predictive of CRC development in a testing cohort (receiver operating characteristic area under the curve, ROCAUC: 0.76, 95% confidence interval: 0.71-0.81). This model has the potential to improve early diagnosis of CRC, particularly in cases of patient noncompliance with FIT.
© 2024. The Author(s).
Conflict of interest statement
Figures


References
-
- Cancer Research UK. Cancer mortality for common cancers. 2022. https://www.cancerresearchuk.org/health-professional/cancer-statistics/m....
-
- Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. 2019;16:713–32. - PubMed
-
- Cancer Research UK. Early Diagnosis Data Hub. 2022. https://crukcancerintelligence.shinyapps.io/EarlyDiagnosis/.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
