

Automated evaluation of diaphragm configuration based on chest CT in COPD patients
- PMID: 39090324
- PMCID: PMC11294507
- DOI: 10.1186/s41747-024-00491-9
Automated evaluation of diaphragm configuration based on chest CT in COPD patients
Abstract
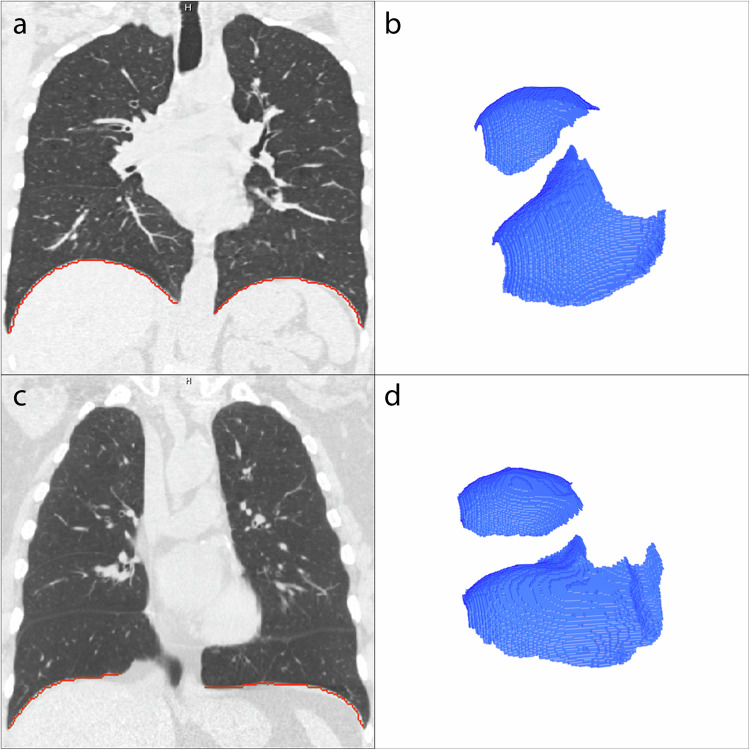
Background: Severe chronic obstructive pulmonary disease (COPD) often results in hyperinflation and flattening of the diaphragm. An automated computed tomography (CT)-based tool for quantifying diaphragm configuration, a biomarker for COPD, was developed in-house and tested in a large cohort of COPD patients.
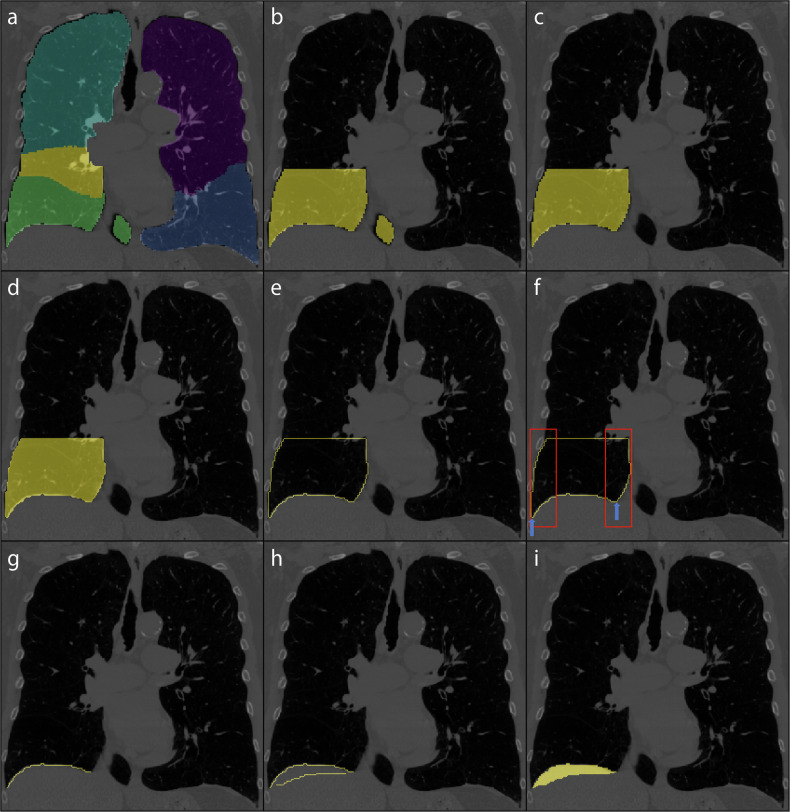
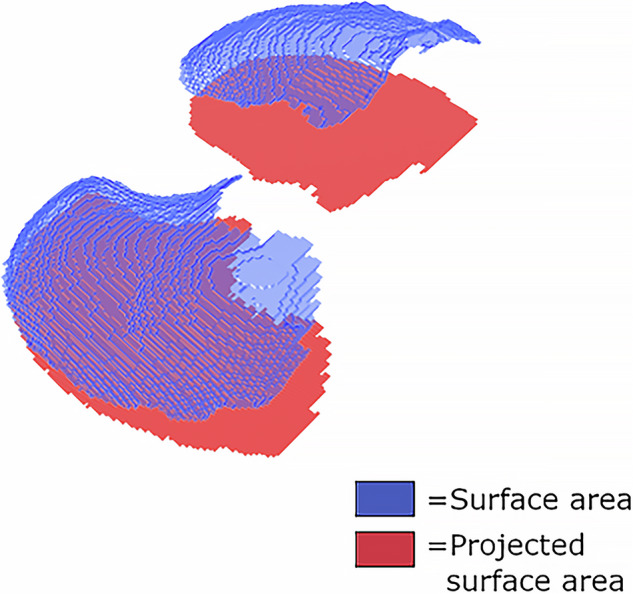
Methods: We used the LungQ platform to extract the lung-diaphragm intersection, as direct diaphragm segmentation is challenging. The tool computed the diaphragm index (surface area/projected surface area) as a measure of diaphragm configuration on inspiratory scans in a COPDGene subcohort. Visual inspection of 250 randomly selected segmentations served as a quality check. Associations between the diaphragm index, Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages, forced expiratory volume in 1 s (FEV1) % predicted, and CT-derived emphysema scores were explored using analysis of variance and Pearson correlation.
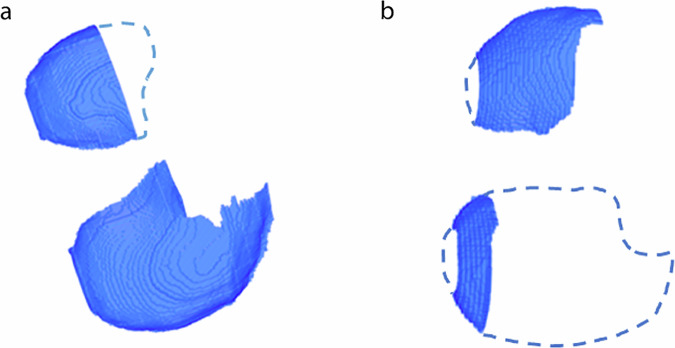
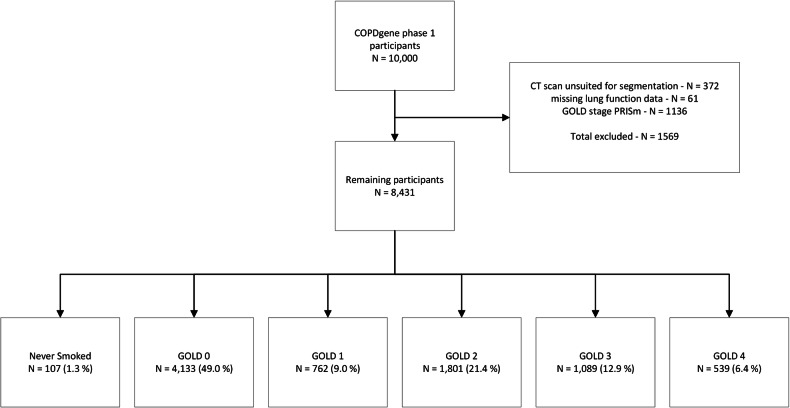
Results: The tool yielded incomplete segmentation in 9.2% (2.4% major defect, 6.8% minor defect) of 250 randomly selected cases. In 8431 COPDGene subjects (4240 healthy; 4191 COPD), the diaphragm index was increasingly lower with higher GOLD stages (never-smoked 1.83 ± 0.16; GOLD-0 1.79 ± 0.18; GOLD-1 1.71 ± 0.15; GOLD-2: 1.67 ± 0.16; GOLD-3 1.58 ± 0.14; GOLD-4 1.54 ± 0.11) (p < 0.001). Associations were found between the diaphragm index and both FEV1% predicted (r = 0.44, p < 0.001) and emphysema score (r = -0.36, p < 0.001).
Conclusion: We developed an automated tool to quantify the diaphragm configuration in chest CT. The diaphragm index was associated with COPD severity, FEV1%predicted, and emphysema score.
Relevance statement: Due to the hypothesized relationship between diaphragm dysfunction and diaphragm configuration in COPD patients, automatic quantification of diaphragm configuration may prove useful in evaluating treatment efficacy in terms of lung volume reduction.
Key points: Severe COPD changes diaphragm configuration to a flattened state, impeding function. An automated tool quantified diaphragm configuration on chest-CT providing a diaphragm index. The diaphragm index was correlated to COPD severity and may aid treatment assessment.
Keywords: Diaphragm; Lung pulmonary disease (chronic obstructive); Segmentation tool; Tomography (x-ray computed).
© 2024. The Author(s).
Conflict of interest statement
DJS is an advisor to Thirona, Nijmegen, NL. RV has received institutional research grants from Siemens Healthineers. MT is employed by Thirona, Nijmegen, NL. JPC is employed by Thirona, Nijmegen, NL, and is a shareholder of Thirona, Nijmegen, NL. All other authors have no competing interests to declare.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical