

Malaria community case management usage and quality of malaria care in a moderate Plasmodium falciparum burden region of Chadiza District, Zambia
- PMID: 39090589
- PMCID: PMC11292954
- DOI: 10.1186/s12936-024-05047-1
Malaria community case management usage and quality of malaria care in a moderate Plasmodium falciparum burden region of Chadiza District, Zambia
Abstract
Background: Malaria community case management (CCM) can improve timely access to healthcare, and CCM programmes in sub-Saharan Africa are expanding from serving children under 5 years (CU5) only to all ages. This report characterizes malaria case management in the setting of an age-expanded CCM programme in Chadiza District, Zambia.
Methods: Thirty-three households in each of 73 eligible communities were randomly selected to participate in a household survey preceding a trial of proactive CCM (NCT04839900). All household members were asked about fever in the prior two weeks and received a malaria rapid diagnostic test (RDT); those reporting fever were asked about healthcare received. Weighted population estimates were calculated and mixed effects regression was used to assess factors associated with malaria care seeking.
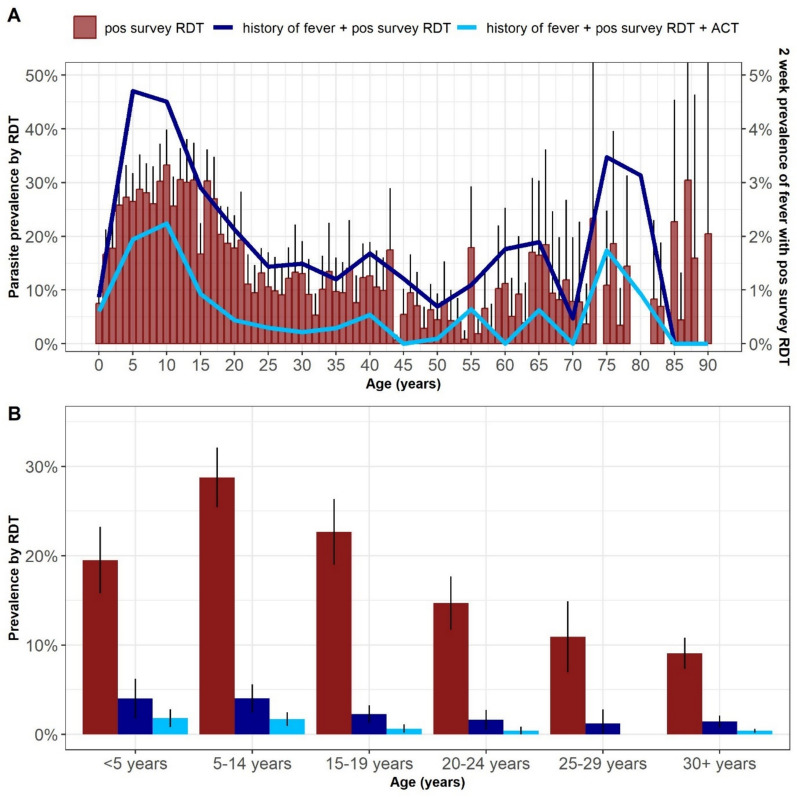
Results: Among 11,030 (98.6%) participants with RDT results (2,357 households), parasite prevalence was 19.1% by RDT; school-aged children (SAC, 5-14 years) had the highest prevalence (28.8%). Prior fever was reported by 12.4% of CU5, 7.5% of SAC, and 7.2% of individuals ≥ 15 years. Among those with prior fever, 34.0% of CU5, 56.0% of SAC, and 22.6% of individuals ≥ 15 years had a positive survey RDT and 73.7% of CU5, 66.5% of SAC, and 56.3% of individuals ≥ 15 years reported seeking treatment; 76.7% across all ages visited a CHW as part of care. Nearly 90% (87.8%) of people who visited a CHW reported a blood test compared with 73.5% seen only at a health facility and/or pharmacy (p < 0.001). Reported malaria treatment was similar by provider, and 85.9% of those with a reported positive malaria test reported getting malaria treatment; 66.9% of the subset with prior fever and a positive survey RDT reported malaria treatment. Age under 5 years, monthly or more frequent CHW home visits, and greater wealth were associated with increased odds of receiving healthcare.
Conclusions: Chadiza District had high CHW coverage among individuals who sought care for fever. Further interventions are needed to increase the proportion of febrile individuals who receive healthcare. Strategies to decrease barriers to healthcare, such as CHW home visits, particularly targeting those of all ages in lower wealth strata, could maximize the benefits of CHW programmes.
Keywords: Plasmodium falciparum prevalence; Community health workers; Healthcare seeking; Malaria; Malaria case management.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Sayre D, Steinhardt LC, Irinantenaina J, Dentinger C, Rasoanaivo TF, Kapesa L, et al. Baseline malaria prevalence and care-seeking behaviours in rural Madagascar prior to a trial to expand malaria community case management to all ages. Malar J. 2021;20:422. 10.1186/s12936-021-03956-z - DOI - PMC - PubMed
-
- Uwimana A, Penkunas MJ, Nisingizwe MP, Uyizeye D, Hakizimana D, Musanabaganwa C, et al. Expanding home-based management of malaria to all age groups in Rwanda: analysis of acceptability and facility-level time-series data. Trans R Soc Trop Med Hyg. 2018;112:513–21. 10.1093/trstmh/try093 - DOI - PubMed
-
- Bennett A, Bisanzio D, Yukich JO, Mappin B, Fergus CA, Lynch M, et al. Population coverage of artemisinin-based combination treatment in children younger than 5 years with fever and Plasmodiumfalciparum infection in Africa, 2003–2015: a modelling study using data from national surveys. Lancet Glob Health. 2017;5:e418–27. 10.1016/S2214-109X(17)30076-1 - DOI - PMC - PubMed
-
- WHO. World Malaria Report 2023. Geneva: World Health Organization; 2023.
MeSH terms
LinkOut - more resources
Full Text Sources
