

Pediatric TBI: Direct admissions vs. secondary referrals to a hospital: A single‑center, retrospective study
- PMID: 39092010
- PMCID: PMC11289858
- DOI: 10.3892/mi.2024.182
Pediatric TBI: Direct admissions vs. secondary referrals to a hospital: A single‑center, retrospective study
Abstract
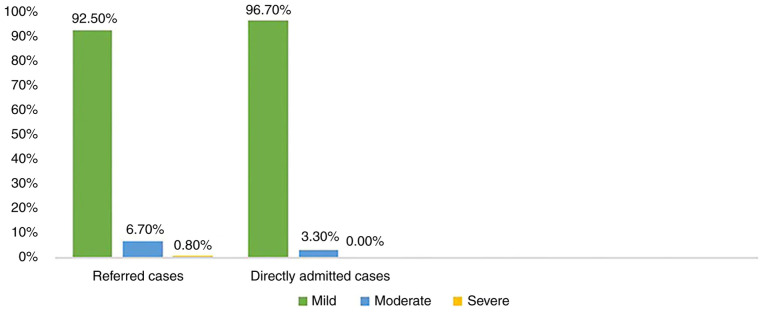
The present retrospective study was conducted in an aim to examine the differences between pediatric traumatic brain injury (TBI) cases referred to and those admitted directly to the hospital. For this purpose, pediatric patients who presented to a main trauma center with TBI between January, 2015 and December, 2019 were reviewed retrospectively, emphasizing whether they were admitted directly or referred from another center. Data collected included the demographic characteristics of the patients, as well as their presenting complaints and the cause of TBI. A total of 981 cases of pediatric TBI were admitted over the 5-year period. The average age of the patients was 58.1 months for the referred cases and almost 50 months for the patients directly admitted. The male sex accounted for 63.6% of all cases. The most common cause of injury was falling (63.5%). Nausea and vomiting were the most typical presenting symptoms, occurring more among the directly admitted cases (P-value ≤0.05). Mild TBI accounted for 85.3% of the cases, and the most common radiological diagnosis was skull fracture (37.4%) (P-value ≤0.004). The referred patients had a more extended hospital stay (P-value ≤0.001). On the whole, the present study identified 981 cases; the majority of these were direct admissions, and the majority of the severe cases were referred from other healthcare facilities. Further research is required on this topic as only a single hospital was covered herein, and patients were not followed-up after discharge. A multi-center analysis would cover a greater number of patients and would thus provide more substantial data on the topic.
Keywords: interhospital; pediatric; traumatic brain injury.
Copyright: © 2024 Allawati et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gardner MT, O'Meara AMI, Ferguson NM. Pediatric traumatic brain injury: An update on management. Curr Pediatr Rep. 2017;5:213–219.
-
- Anderson V, Moore C. Age at injury as a predictor of outcome following pediatric head injury: A longitudinal perspective. Child Neuropsychol. 1995;1:187–202.
LinkOut - more resources
Full Text Sources