

Association between polymorphisms of DNA repair genes and intracranial aneurysms: A systematic review and meta‑analysis
- PMID: 39092011
- PMCID: PMC11289859
- DOI: 10.3892/mi.2024.183
Association between polymorphisms of DNA repair genes and intracranial aneurysms: A systematic review and meta‑analysis
Abstract
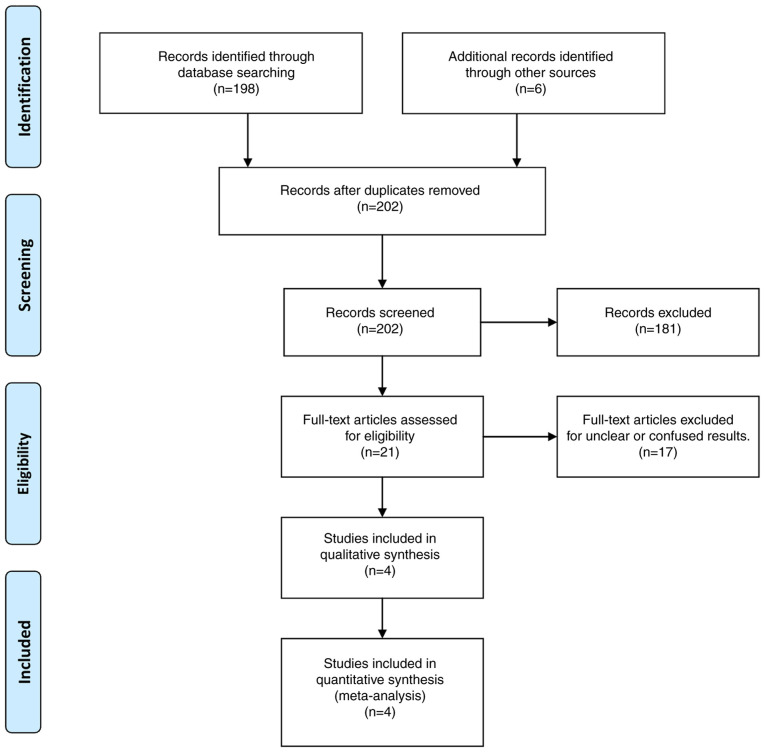
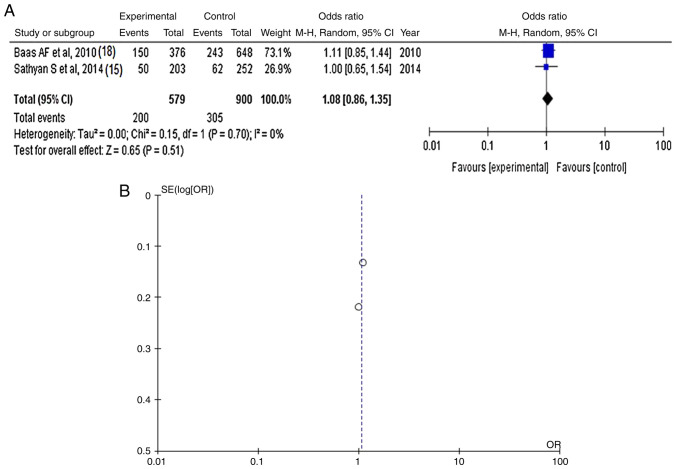
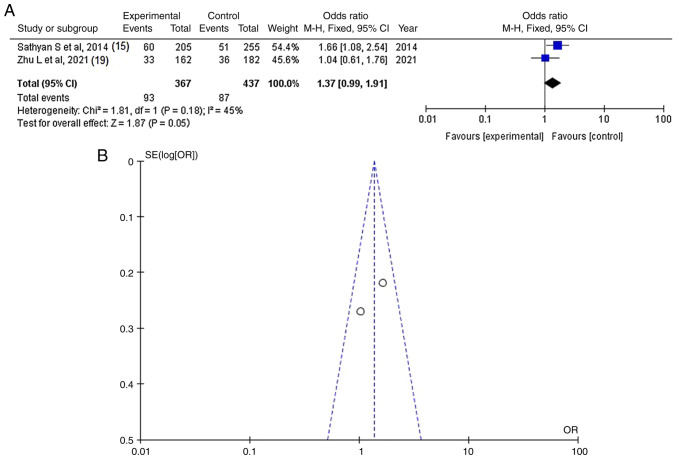
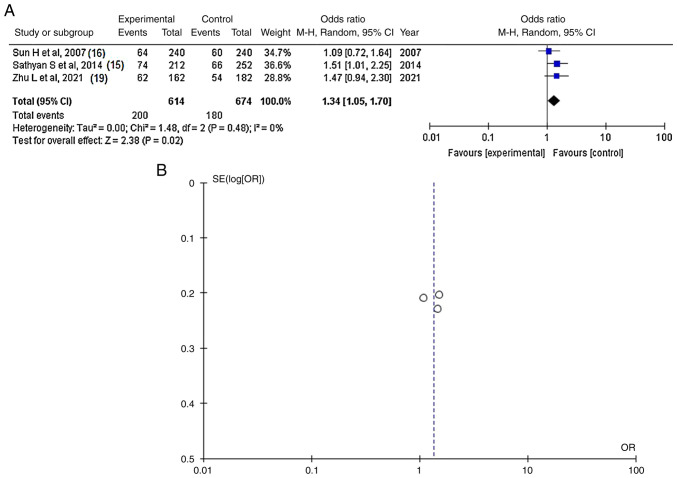
Intracranial aneurysms (IAs) are present in ~2% of the general population, and genetic factors cannot be excluded for the risk of their development. The gene factors that result in the changes in the vascular extracellular matrix (ECM) may also be a key reason for IAs being hereditary. The VCAN gene [also known as chondroitin sulfate proteoglycan 2 (CSPG2)] plays various roles in maintaining ECM functions. The present systematic review and meta-analysis aimed to investigate all eligible articles involving IAs on the association with germ line SNPs of DNA repair genes (up to January, 2024). The total number of patients was 2,308 [987 cases (poor outcomes) and 1,321 controls (good outcomes)]. The results revealed that rs2287926 G/G genotype and G allele and rs251124 T/T genotype and minor allele T increased the risk of developing IAs. However, further studies are required to examine these gene polymorphisms as screening markers for IAs.
Keywords: aneurysms; chondroitin sulfate proteoglycan 2 gene; gene associations; intracranial aneurysms; single nucleotide polymorphisms.
Copyright: © 2024 Montasr et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
The Association between Genes Polymorphisms of Heparan Sulfate Proteoglycan 2 (HSPG2) and Chondroitin Sulfate Proteoglycan 2 (CSPG2) and Intracranial Aneurysm Susceptibility: A Meta-Analysis.Iran J Public Health. 2019 Nov;48(11):1945-1951. Iran J Public Health. 2019. PMID: 31970092 Free PMC article. Review.
-
Association of Versican Gene Polymorphisms with Intracranial Aneurysm Susceptibility in the Eastern Chinese Population.Neuropsychiatr Dis Treat. 2021 Dec 7;17:3531-3537. doi: 10.2147/NDT.S338311. eCollection 2021. Neuropsychiatr Dis Treat. 2021. PMID: 34908835 Free PMC article.
-
Chondroitin sulfate proteoglycan 2 (CSPG2) gene polymorphisms rs173686 and rs251124 are not associated with intracranial aneurysms in Chinese Han nationality.Ups J Med Sci. 2007;112(3):289-95. doi: 10.3109/2000-1967-201. Ups J Med Sci. 2007. PMID: 18484070
-
Association of Versican (VCAN) gene polymorphisms rs251124 and rs2287926 (G428D), with intracranial aneurysm.Meta Gene. 2014 Sep 14;2:651-60. doi: 10.1016/j.mgene.2014.07.001. eCollection 2014 Dec. Meta Gene. 2014. PMID: 25606449 Free PMC article.
-
Collagen type-I A2 gene polymorphisms and susceptibility to intracranial aneurysms: a meta-analysis of genetic association studies.Int J Neurosci. 2018 Jul;128(7):640-653. doi: 10.1080/00207454.2017.1408616. Epub 2017 Dec 13. Int J Neurosci. 2018. PMID: 29164999 Review.
References
LinkOut - more resources
Full Text Sources