

Insulin sensitivity, disposition index and insulin clearance in cystic fibrosis: a cross-sectional study
- PMID: 39093413
- PMCID: PMC11447061
- DOI: 10.1007/s00125-024-06220-6
Insulin sensitivity, disposition index and insulin clearance in cystic fibrosis: a cross-sectional study
Abstract
Aims/hypothesis: The aim of this study was to investigate insulin secretion, insulin sensitivity, disposition index and insulin clearance by glucose tolerance status in individuals with cystic fibrosis (CF) and exocrine pancreatic insufficiency.
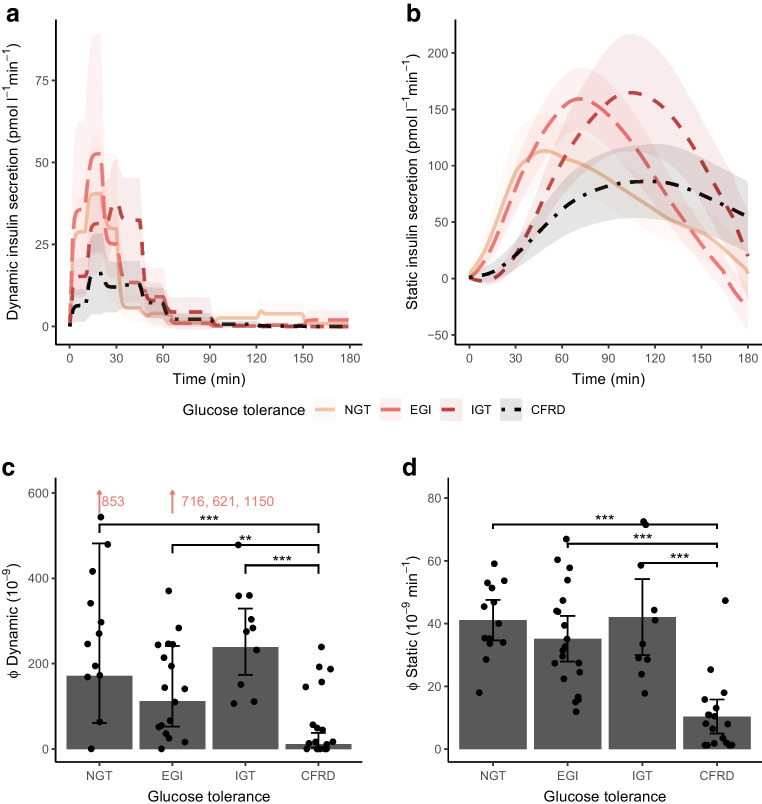
Methods: In a cross-sectional study, we conducted an extended (ten samples) OGTT in individuals with pancreatic-insufficient CF (PI-CF). Participants were divided into normal glucose tolerance (NGT), early glucose intolerance (EGI), impaired glucose tolerance (IGT) and CF-related diabetes (CFRD) groups. We used three different oral minimal models to assess insulin secretion, insulin sensitivity and insulin clearance during the OGTT. We evaluated insulin secretion using total secretion (Φ total), first-phase secretion (Φ dynamic) and second-phase secretion (Φ static) from the model, and we estimated the disposition index by multiplying Φ total and insulin sensitivity.
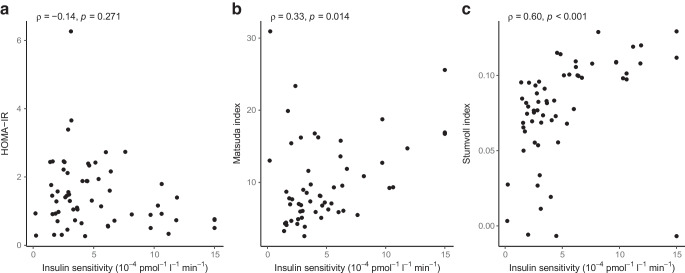
Results: Among 61 participants (NGT 21%, EGI 33%, IGT 16%, CFRD 30%), insulin secretion indices (Φ total, dynamic and static) were significantly lower in the CFRD group compared with the other groups. Insulin sensitivity declined with worsening in glucose tolerance (p value for trend <0.001) and the disposition index declined between NGT and EGI and between IGT and CFRD. Those with CFRD had elevated insulin clearance compared with NGT (p=0.019) and low insulin secretion (Φ total) was also associated with high insulin clearance (p<0.001).
Conclusions/interpretation: In individuals with PI-CF, disposition index declined with incremental impairment in glucose tolerance due to a reduction in both insulin secretion and insulin sensitivity. Moreover in CF, reduced insulin secretion was associated with higher insulin clearance.
Keywords: CFRD; Disposition index; Insulin clearance; Insulin secretion; Insulin sensitivity; Minimal models.
© 2024. The Author(s).
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
