

Multicenter and inter-software evaluation of ablative margins after thermal ablation of colorectal liver metastases
- PMID: 39093415
- PMCID: PMC11782453
- DOI: 10.1007/s00330-024-10956-5
Multicenter and inter-software evaluation of ablative margins after thermal ablation of colorectal liver metastases
Abstract
Purpose: To assess the association between minimal ablative margin (MAM) and local tumor progression (LTP) following CT-guided thermal ablation of colorectal liver metastases (CRLM) in a multicenter cohort and across two confirmation software.
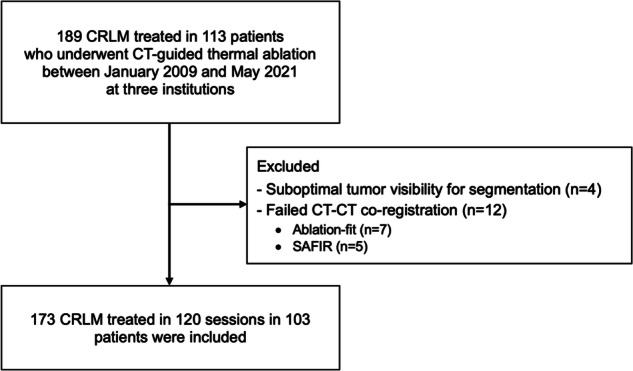
Materials and methods: This multicenter retrospective study included patients who underwent CT-guided radiofrequency or microwave ablation for CRLM between 2009 and 2021 in three institutions. Three-dimensional (3D) MAM was retrospectively assessed using dedicated ablation confirmation software by automatic non-rigid (Ablation-fit) or semi-automatic rigid co-registration (SAFIR) of intraprocedural pre- and post-ablation contrast-enhanced CT scans by two independent reader teams blinded to patient outcomes. LTP was assessed on a per-tumor basis. Factors associated with LTP-free survival were assessed using multivariable Cox regression analysis.
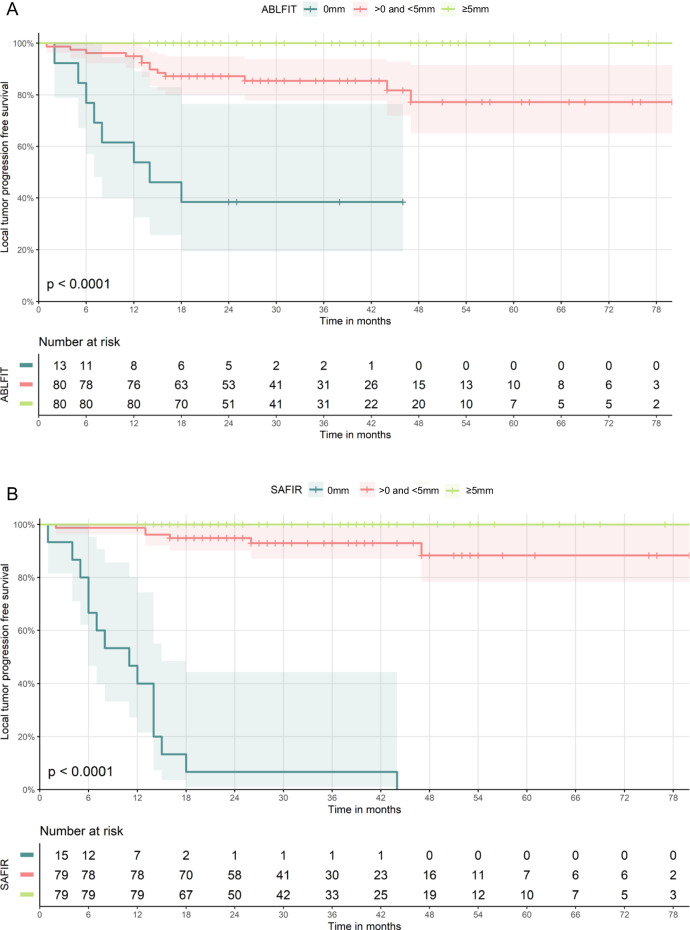
Results: Overall, 113 patients (mean age: 67 ± 10 years; 78 men) who underwent thermal ablation for 189 CRLM (mean diameter: 1.9 ± 1.1 cm) met the inclusion criteria. 173/189 (92%) CRLM could be successfully analyzed using both software. Over a median follow-up of 31 months (IQR: 22-47), 21 of 173 CRLM (12.1%) developed LTP. On multivariable analysis, 3D MAM was independently associated with LTP in both software (Ablation-fit: HR 0.47, 95% CI: 0.36-0.61, p < 0.001; SAFIR: HR 0.42, 95% CI: 0.32-0.55, p < 0.001). No LTP was observed in CRLM ablated with MAM ≥ 4 mm (Ablation-fit) and ≥ 5 mm (SAFIR). The per-tumor median absolute difference in MAM quantification between both software was 2 mm (IQR: 1-3).
Conclusion: MAM was independently associated with LTP after thermal ablation of CRLM across multicenter data and two confirmation software. Ablations achieving a MAM ≥ 5 mm were associated with local control in both software.
Clinical relevance statement: MAMs from intraprocedural contrast-enhanced CT were independently associated with LTP after thermal ablation of CRLM across multicenter data and two confirmation software, with a margin ≥ 5 mm associated with local control in both software.
Key points: Sufficient ablative margins are critical for local control following thermal ablation of CRLM. Intraprocedural CT-derived MAM was the only independent factor associated with LTP across two confirmation software. No LTP was observed in CRLM ablated with a MAM ≥ 5 mm.
Keywords: Imaging (three-dimensional); Liver neoplasms; Radiofrequency ablation; Treatment outcome.
© 2024. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is Dr. Christiaan G. Overduin. Conflict of interest: The authors of this manuscript declare relationships with the following companies: M.R.M. Medtronic-Covidien, Johnson & Johnson, Angiodynamics, Philips, Immunophotonics, and Guerbet. R.B. with Interventional Systems. The remaining authors declare no conflicts of interest. Statistics and biometry: One of the authors has significant statistical expertise. Informed consent: Only if the study is on human subjects: written informed consent was waived by the Institutional Review Board. For this retrospective study, informed consent to use and exchange pseudonymized data was waived by the local institutional review board at each institution (2018–2053; 2020.077; 1316/2021) for all study participants. All data was shared under data sharing agreements (A20-0423; A21-0442) in compliance with local regulations. Ethical approval: Institutional Review Board approval was obtained. Study subjects or cohorts overlap: In a prior study (Laimer 2021—PMID: 33447860), we reported on 45 of 113 patients included in the current study. The previous study was a single-center study utilizing one confirmation software (Ablation-fit). The current study expands on this by having a multicenter cohort and all data analyzed by a second confirmation software, providing a significantly increased study population and additional and new analyses per software, including inter-software agreement. The extent of overlap has been explicitly mentioned in the Materials and Methods section of the manuscript (Page 4, 1st paragraph), including reference to the prior study. Methodology: Retrospective Observational Multicenter study
Figures


Comment in
-
Automated evaluation of ablative margins in thermal ablation: more evidence for the clinical impact of computer science, onward to enhanced needle placement.Eur Radiol. 2025 Feb;35(2):1044-1045. doi: 10.1007/s00330-024-11090-y. Epub 2024 Sep 26. Eur Radiol. 2025. PMID: 39325183 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
