

Preoperative Chemoradiotherapy vs Chemotherapy for Adenocarcinoma of the Esophagogastric Junction: A Network Meta-Analysis
- PMID: 39093560
- PMCID: PMC11297377
- DOI: 10.1001/jamanetworkopen.2024.25581
Preoperative Chemoradiotherapy vs Chemotherapy for Adenocarcinoma of the Esophagogastric Junction: A Network Meta-Analysis
Erratum in
-
Errors in Figure 3.JAMA Netw Open. 2025 Sep 2;8(9):e2535510. doi: 10.1001/jamanetworkopen.2025.35510. JAMA Netw Open. 2025. PMID: 40932725 Free PMC article. No abstract available.
Abstract
Importance: The prognosis of patients with adenocarcinoma of the esophagus and esophagogastric junction (AEG) is poor. From current evidence, it remains unclear to what extent preoperative chemoradiotherapy (CRT) or preoperative and/or perioperative chemotherapy achieve better outcomes than surgery alone.
Objective: To assess the association of preoperative CRT and preoperative and/or perioperative chemotherapy in patients with AEG with overall survival and other outcomes.
Data sources: Literature search in PubMed, Cochrane Library, Cumulative Index to Nursing and Allied Health Literature, ClinicalTrials.gov, and International Clinical Trials Registry Platform was performed from inception to April 21, 2023.
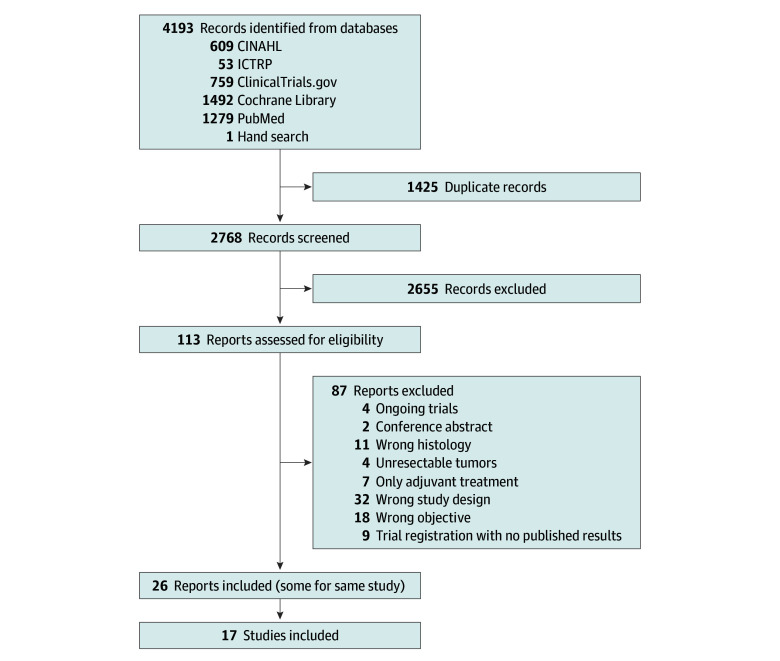
Study selection: Two blinded reviewers screened for randomized clinical trials comparing preoperative CRT plus surgery with preoperative and/or perioperative chemotherapy plus surgery, 1 intervention with surgery alone, or all 3 treatments. Only data from participants with AEG were included from trials that encompassed mixed histology or gastric cancer. Among 2768 initially identified studies, 17 (0.6%) met the selection criteria.
Data extraction and synthesis: The Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines were followed for extracting data and assessing data quality by 2 independent extractors. A bayesian network meta-analysis was conducted using the 2-stage approach.
Main outcomes and measures: Overall and disease-free survival, postoperative morbidity, and mortality.
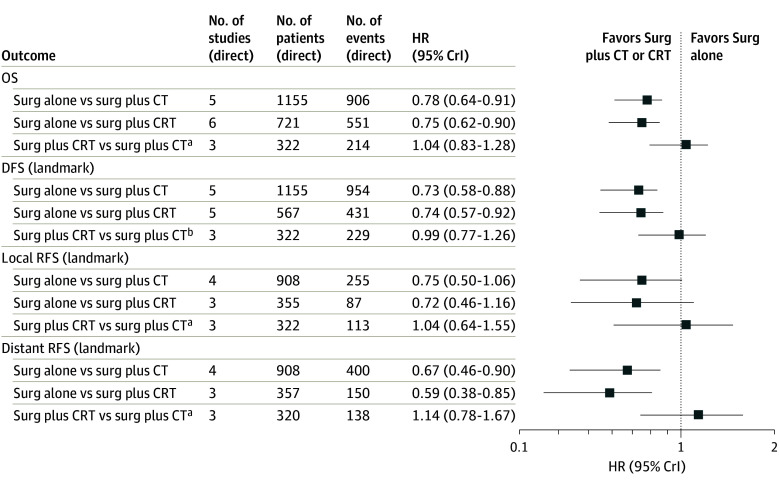
Results: The analyses included 2549 patients (2206 [86.5%] male; mean [SD] age, 61.0 [9.4] years) from 17 trials (conducted from 1989-2016). Both preoperative CRT plus surgery (hazard ratio [HR], 0.75 [95% credible interval (CrI), 0.62-0.90]; 3-year difference, 105 deaths per 1000 patients) and preoperative and/or perioperative chemotherapy plus surgery (HR, 0.78 [95% CrI, 0.64-0.91]; 3-year difference, 90 deaths per 1000 patients) showed longer overall survival than surgery alone. Comparing the 2 modalities yielded similar overall survival (HR, 1.04 [95% CrI], 0.83-1.28]; 3-year difference, 15 deaths per 1000 patients fewer for CRT). Similarly, disease-free survival was longer for both modalities compared with surgery alone. Postoperative morbidity was more frequent after CRT plus surgery (odds ratio [OR], 2.94 [95% CrI, 1.01-8.59]) than surgery alone. Postoperative mortality was not significantly more frequent after CRT plus surgery than surgery alone (OR, 2.50 [95% CrI, 0.66-10.56]) or after chemotherapy plus surgery than CRT plus surgery (OR, 0.44 [95% CrI, 0.08-2.00]).
Conclusions and relevance: In this meta-analysis of patients with AEG, both preoperative CRT and preoperative and/or perioperative chemotherapy were associated with longer survival without relevant differences between the 2 modalities. Thus, either of the 2 treatments may be recommended to patients.
Conflict of interest statement
Figures

References
-
- Morgan E, Soerjomataram I, Rumgay H, et al. The global landscape of esophageal squamous cell carcinoma and esophageal adenocarcinoma incidence and mortality in 2020 and projections to 2040: new estimates from GLOBOCAN 2020. Gastroenterology. 2022;163(3):649-658.e2. doi: 10.1053/j.gastro.2022.05.054 - DOI - PubMed
-
- Ronellenfitsch U, Schwarzbach M, Hofheinz R, et al. Preoperative chemo(radio)therapy versus primary surgery for gastroesophageal adenocarcinoma: systematic review with meta-analysis combining individual patient and aggregate data. Eur J Cancer. 2013;49(15):3149-3158. doi: 10.1016/j.ejca.2013.05.029 - DOI - PubMed
-
- Sjoquist KM, Burmeister BH, Smithers BM, et al. ; Australasian Gastro-Intestinal Trials Group . Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011;12(7):681-692. doi: 10.1016/S1470-2045(11)70142-5 - DOI - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
