

A preliminary investigation into the impact of soft tissue augmentation-based periodontal phenotype modification therapy for patients exhibiting class III decompensation
- PMID: 39095718
- PMCID: PMC11297605
- DOI: 10.1186/s12903-024-04630-x
A preliminary investigation into the impact of soft tissue augmentation-based periodontal phenotype modification therapy for patients exhibiting class III decompensation
Abstract
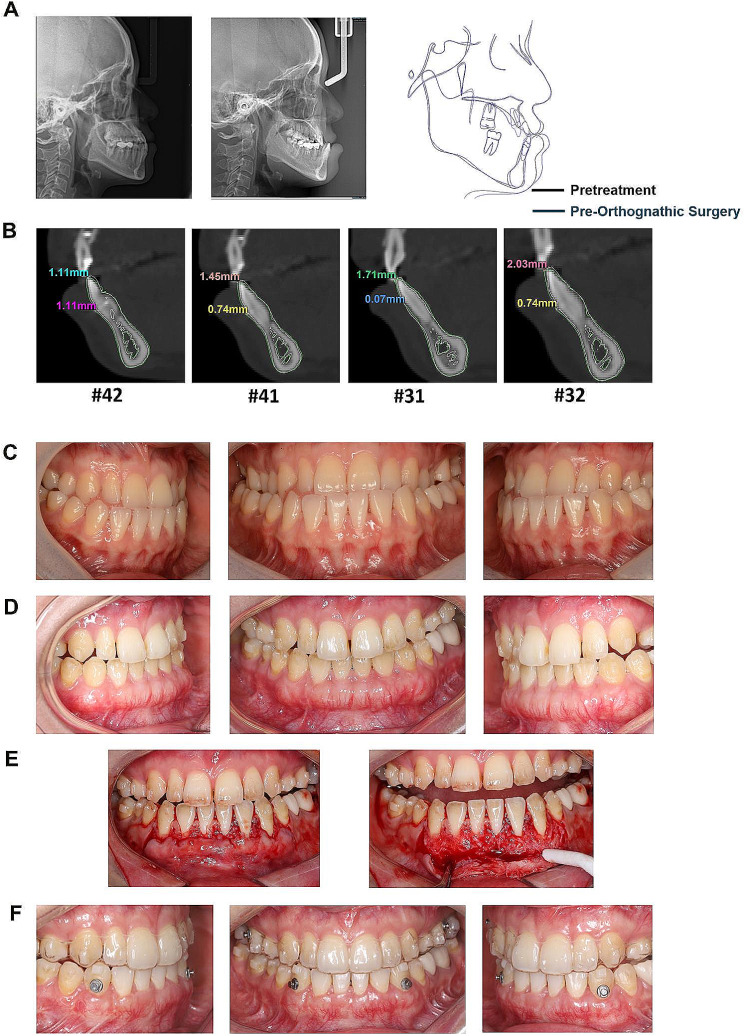
Background: Patients with skeletal angle Class III malocclusion usually have inadequate hard and soft tissue volume at the mandibular anterior teeth. The labial proclination at the teeth may lead to gingival recession. The purpose of this study was to explore whether periodontal phenotype modification therapy with soft tissue augmentation (PhMT-s) can prevent gingival recession in these patients.
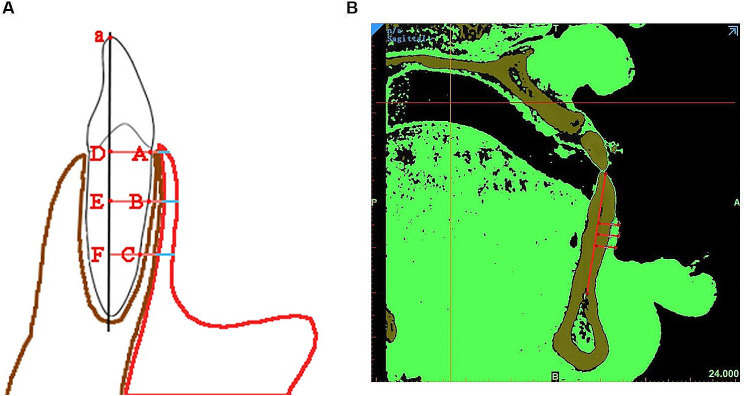
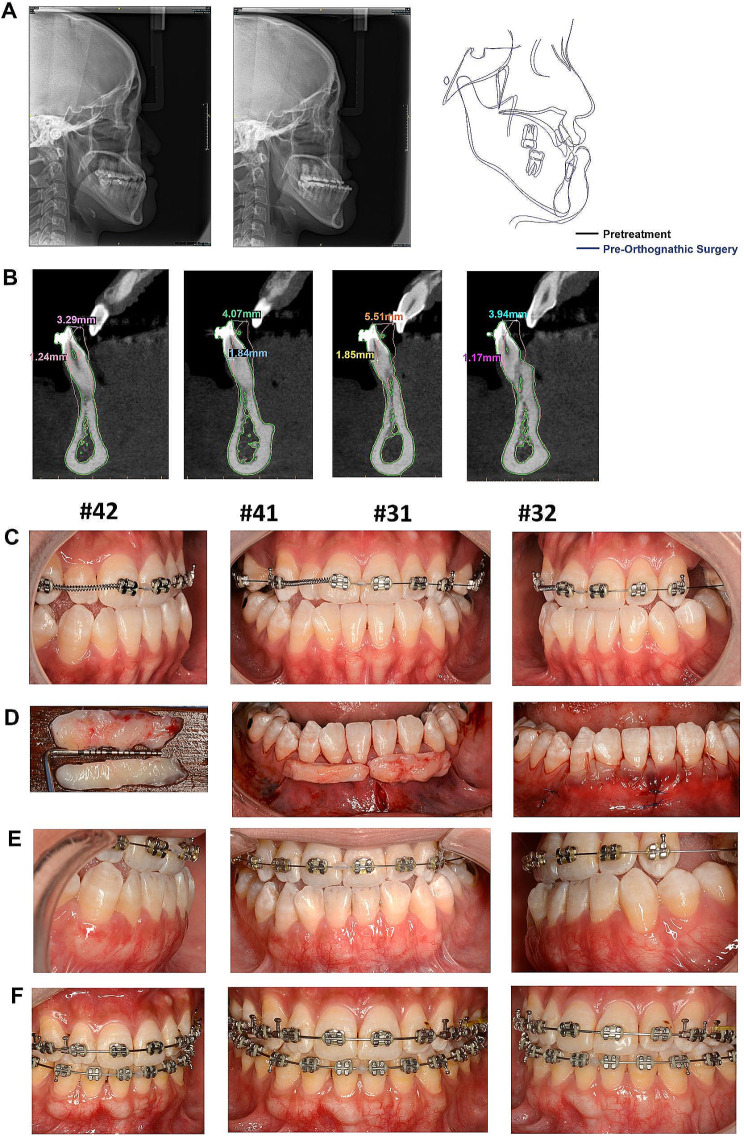
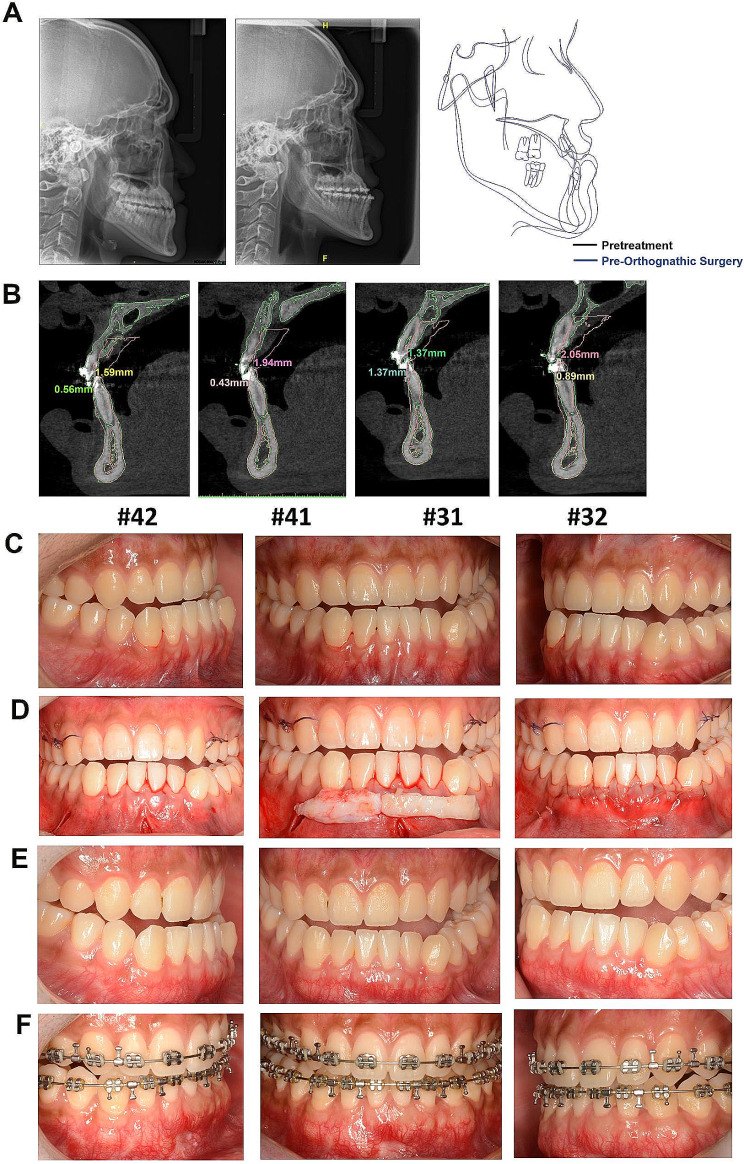
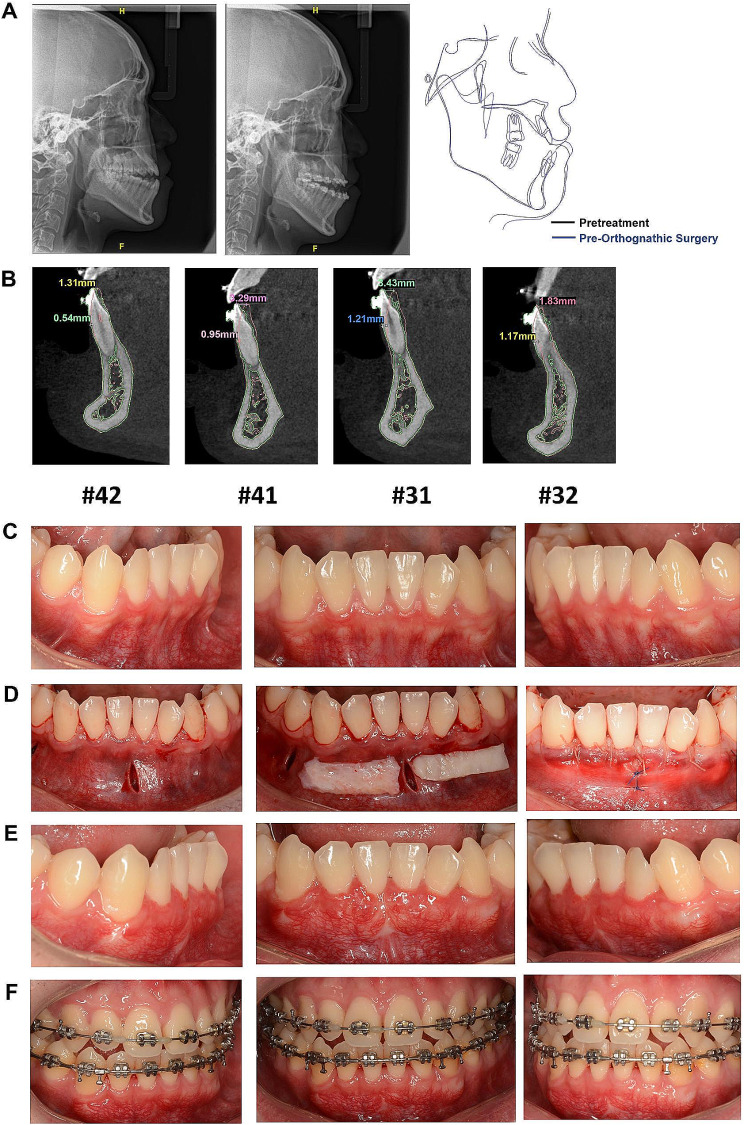
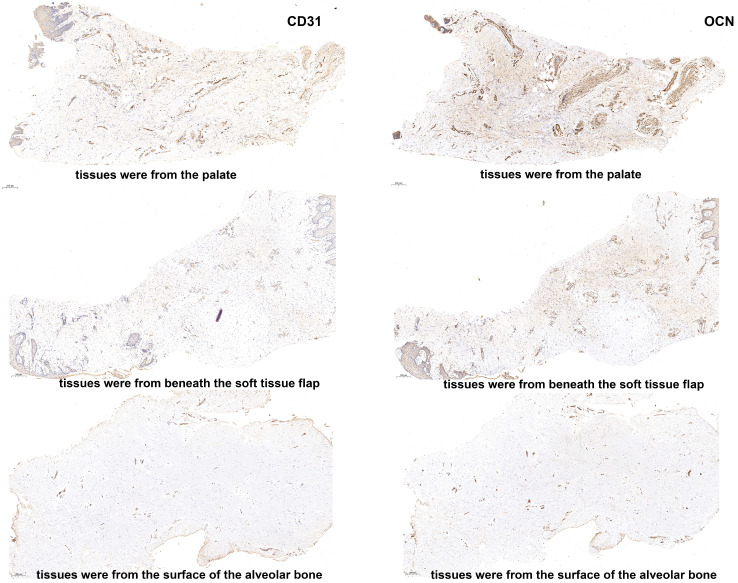
Methods: Four patients with skeletal Class III malocclusion and a thin periodontal phenotype underwent surgical-orthodontic treatment. Prior to tooth movement, they underwent a minimally invasive vestibular incision with subperiosteal tunnel access combined with autogenous connective tissue grafts for periodontal phenotype modification with soft tissue augmentation (PhMT-s). The labial gingival thickness of the anterior mandibular teeth was measured at three distinct levels: at the cementoenamel junction (GT0), 3 mm apical to the CEJ (GT3), and 6 mm apical to the CEJ (GT6). These measurements were taken at baseline, three months following PhMT-s, and after tooth decompensation. Additionally, a biopsy sample was obtained from the PhMT-s site of one patient. All sections were subsequently stained using hematoxylin and eosin, Masson trichrome, Sirius Red, and immunohistochemistry.
Results: The thickness of the labial gingiva was increased about 0.42 to 2.00 mm after PhMT-s. At the end of pre-orthognathic surgical orthodontic treatment, the thickness of the labial gingiva was increased about - 0.14 to 1.32 mm compared to the baseline and no gingival recession occurred after the pre-orthognathic surgical orthodontic treatment. The histologic results demonstrated that the grafts obtained from the PhMT-s site exhibited increased deposition of collagen fibers. Moreover, the proportion of type III collagen increased and the grafts displayed significantly reduced positive expression of CD31 and OCN.
Conclusions: PhMT-s increased the thickness of the soft tissue, stabilizing the gingival margin for teeth exhibiting a thin periodontal phenotype and undergoing labial movement. This is attributed to the increased deposition of collagen fibers.
Keywords: Gingival recession; Periodontal phenotype modification; Skeletal angle class III malocclusion; Soft tissue augmentation; Soft tissue grafting.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Jing WD, Xu L, Xu X, Hou JX, Li XT. Association between Periodontal Biotype and Clinical parameters: a cross-sectional study in patients with skeletal class III malocclusion. Chin J Dent Res. 2019;22:9–19. - PubMed
MeSH terms
Grants and funding
- NO.82301067/National Natural Science Foundation of China
- NO.82301067/National Natural Science Foundation of China
- NO.82301067/National Natural Science Foundation of China
- NO.82301067/National Natural Science Foundation of China
- NO.82301067/National Natural Science Foundation of China
- JYJC202211/Cross-disciplinary Research Fund of Shanghai Ninth People's Hospital, Shanghai Jiao Tong university School of Medicine
- JYJC202211/Cross-disciplinary Research Fund of Shanghai Ninth People's Hospital, Shanghai Jiao Tong university School of Medicine
- JYJC202211/Cross-disciplinary Research Fund of Shanghai Ninth People's Hospital, Shanghai Jiao Tong university School of Medicine
- JYJC202211/Cross-disciplinary Research Fund of Shanghai Ninth People's Hospital, Shanghai Jiao Tong university School of Medicine
- JYJC202211/Cross-disciplinary Research Fund of Shanghai Ninth People's Hospital, Shanghai Jiao Tong university School of Medicine
- 2022cxy-nj/Teachers Practice Plan of Shanghai University
- 2022cxy-nj/Teachers Practice Plan of Shanghai University
- 2022cxy-nj/Teachers Practice Plan of Shanghai University
- 2022cxy-nj/Teachers Practice Plan of Shanghai University
- 2022cxy-nj/Teachers Practice Plan of Shanghai University
- 201912/Clinical Research Project of Multi-Disciplinary Team, Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine
- 201912/Clinical Research Project of Multi-Disciplinary Team, Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine
- 201912/Clinical Research Project of Multi-Disciplinary Team, Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine
- 201912/Clinical Research Project of Multi-Disciplinary Team, Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine
- 201912/Clinical Research Project of Multi-Disciplinary Team, Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine
LinkOut - more resources
Full Text Sources
