

The landscape of circulating tumor HPV DNA and TTMV-HPVDNA for surveillance of HPV-oropharyngeal carcinoma: systematic review and meta-analysis
- PMID: 39095868
- PMCID: PMC11297591
- DOI: 10.1186/s13046-024-03137-1
The landscape of circulating tumor HPV DNA and TTMV-HPVDNA for surveillance of HPV-oropharyngeal carcinoma: systematic review and meta-analysis
Abstract
Background: Human papilloma virus (HPV) related cancers of the oropharynx are rapidly increasing in incidence and may soon represent the majority of all head and neck cancers. Improved monitoring and surveillance methods are thus an urgent need in public health.
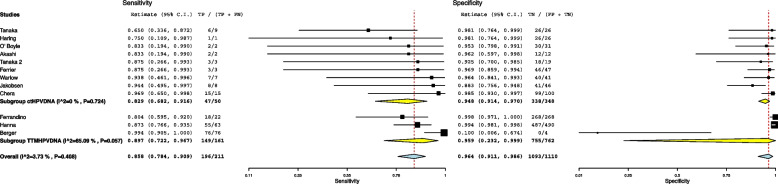
Main text: The goal is to highlight the current potential and limitations of liquid biopsy through a meta analytic study on ctHPVDNA and TTMV-HPVDNA. It was performed a Literature search on articles published until December 2023 using three different databases: MEDLINE, Embase, and Cochrane Library. Studies that evaluated post-treatment ctHPVDNA and TTMV-HPVDNA in patients with HPV + OPSCC, studies reporting complete data on the diagnostic accuracy in recurrence, or in which the number of true positives, false positives, true negatives, and false negatives was extractable, and methods of detection of viral DNA clearly defined. The meta-analysis was conducted following the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) reporting guidelines. The aim of this meta-analysis was to evaluate the sensitivity, specificity, and accuracy of ctHPVDNA and TTMV by ddPCR to define its efficacy in clinical setting for the follow up of HPV-OPSCC.
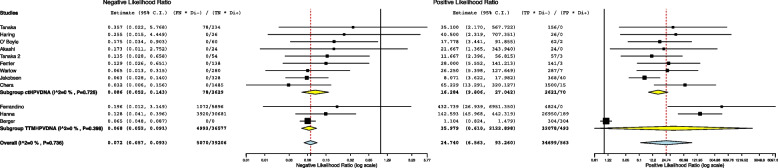
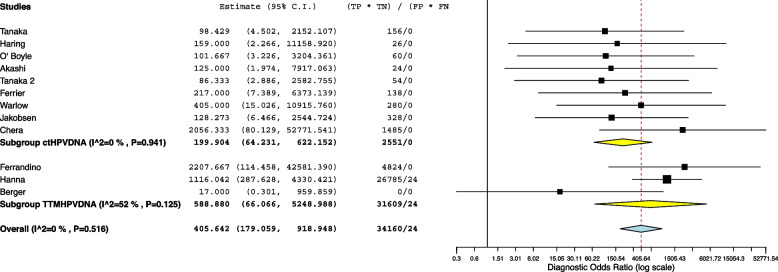
Conclusion: The 12 studies included in the meta-analysis provided a total of 1311 patients for the analysis (398 valuated with ctHPVDNA and 913 with TTMV-HPVDNA). Pooled sensitivity and specificity were 86% (95% CI: 78%-91%) and 96% (95% CI: 91%-99%), respectively; negative and positive likelihood ratios were 0.072 (95% CI: 0.057-0.093) and 24.7 (95% CI: 6.5-93.2), respectively; pooled DOR was 371.66 (95% CI: 179.1-918). The area under the curve (AUC) was 0.81 (95% CI, 0.67-0.91). Liquid biopsy for the identification of cell free DNA might identify earlier recurrence in HPV + OPSCC patients. At the present time, liquid biopsy protocol needs to be standardized and liquid biopsy cannot yet be used in clinical setting. In the future, a multidimensional integrated approach which links multiple clinical, radiological, and laboratory data will contribute to obtain the best follow-up strategies for the follow-up of HPV-OPSCC.
Keywords: Circulating tumour HPVDNA; Follow up; HPV; Liquid biopsy; Oropharyngeal squamous cell carcinoma; TTMV-HPVDNA.
© 2024. The Author(s).
Conflict of interest statement
None of the Authors declared conflict of interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
