

The outcomes of paediatric cataract surgery with intraocular lens insertion in sub-Saharan Africa: a systematic review
- PMID: 39095869
- PMCID: PMC11295353
- DOI: 10.1186/s13643-024-02607-z
The outcomes of paediatric cataract surgery with intraocular lens insertion in sub-Saharan Africa: a systematic review
Abstract
Importance: Cataract is one of the leading causes of childhood blindness in Africa. The management of this condition requires timely surgical extraction of the cataractous lens with immediate optical correction and long-term follow-up to monitor visual improvement and manage complications that may arise. This review provides an opportunity to benchmark outcomes and to shed light on the reasons for those outcomes.
Objectives: To review the published literature and report on the outcomes of paediatric cataract surgery with intraocular lens insertion in sub-Saharan Africa.
Data source: The EMBASE, PubMed, Scopus, and Web of Science were searched for relevant articles.
Study selection: We included all published primary studies from sub-Saharan Africa on cataract surgery outcomes in children aged 0-16 years with primary intraocular lens implantation conducted between 1990 and 2020. Eligible studies were those published in English or for which an English translation was available. In addition, reviewers screened the reference lists of all studies included in the full-text review for eligible studies. During the review, studies fitting the inclusion criteria above except for having been conducted in middle and high-income countries were tagged and placed in a comparison arm.
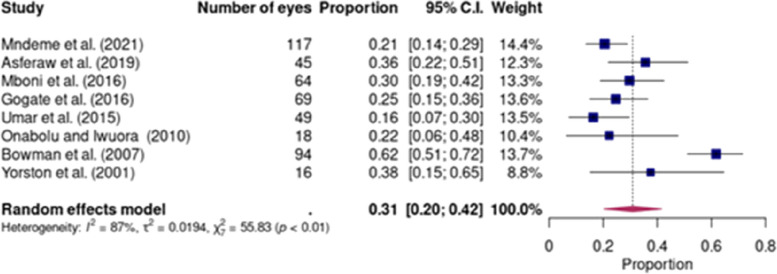
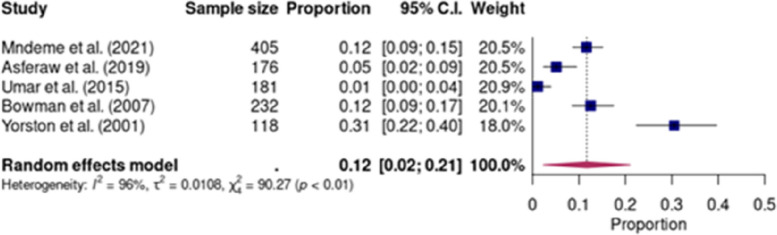
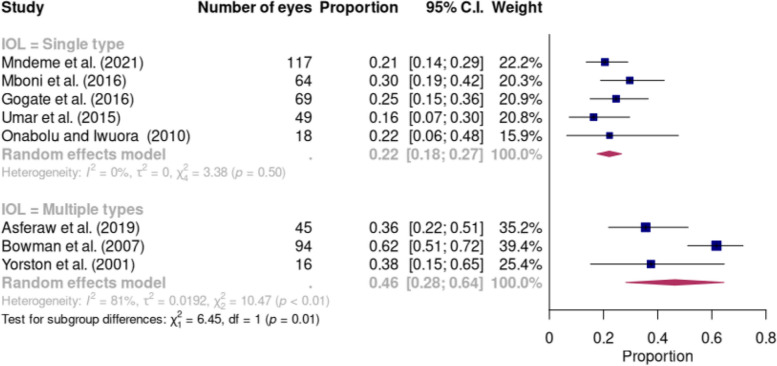
Data extraction and synthesis: Study eligibility was determined by two independent reviewers, and data extraction was conducted by one reviewer with entries checked for accuracy by another reviewer. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines for data synthesis were followed. The Joanna Briggs Institute (JBI) critical appraisal checklist was used for quality appraisal of the studies. The statistical software R was used in the analysis, and data were pooled using a random-effects model. Forest plots were generated using the R package 'metafor'.
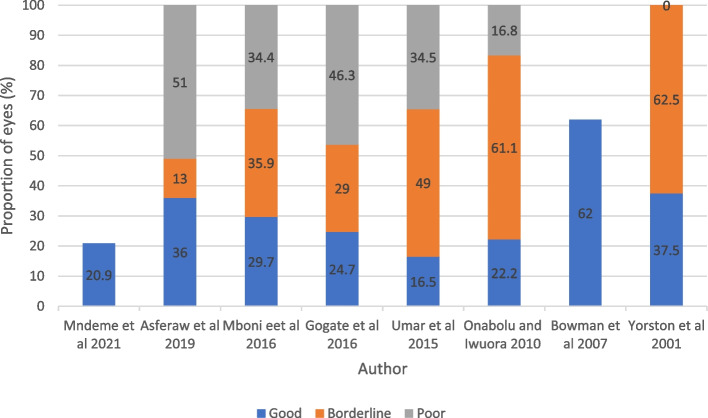
Main outcomes and measures: The primary outcome was visual acuity (VA) after cataract surgery and the proportions of eyes that achieved good, borderline, or poor visual outcome according to the World Health Organisation (WHO) categorisation of post-operative visual acuity. The secondary outcome measures reported included lag time to surgery, rates of follow-up, and rate of complications.
Results: Eight out of 4763 studies were eligible for inclusion in this review, and seven were included in the quantitative analysis. There was a male preponderance in the study population, and the mean age at the time of cataract surgery ranged from 3.4 to 8.4 years. Visual outcomes were available for short-term visual outcomes (1 to 6 months) as the studies had a significant loss to follow-up. The pooled proportion of eyes that achieved a good visual acuity (i.e. equal to or greater than 6/18) in the short-term period was 31% (CI, 20-42). The comparative studies from middle and high-income countries reported proportions ranging from 41 to 91%, with higher thresholds for good visual acuity of 6/12 and 6/15.
Conclusion and relevance: This review reports that there is a lower proportion of eyes with good outcomes after undergoing paediatric cataract surgery in sub-Saharan Africa than in middle- and high-income countries. Furthermore, this review states that there is a high proportion of patients lost to follow-up and suboptimal refractive correction and amblyopia treatment after paediatric cataract surgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Basti S, Greenwald MJ. Principles and paradigms of pediatric cataract management. Indian J Ophthalmol. 1995;43(4):159–76. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
