

"I didn't even wonder why I was on the floor" - mixed methods exploration of stroke awareness and help-seeking behaviour at stroke symptom onset
- PMID: 39095882
- PMCID: PMC11295636
- DOI: 10.1186/s12913-024-11276-6
"I didn't even wonder why I was on the floor" - mixed methods exploration of stroke awareness and help-seeking behaviour at stroke symptom onset
Abstract
Introduction: To better target stroke awareness efforts (pre and post first stroke) and thereby decrease the time window for help-seeking, this study aims to assess quantitatively whether stroke awareness is associated with appropriate help-seeking at symptom onset, and to investigate qualitatively why this may (not) be the case.
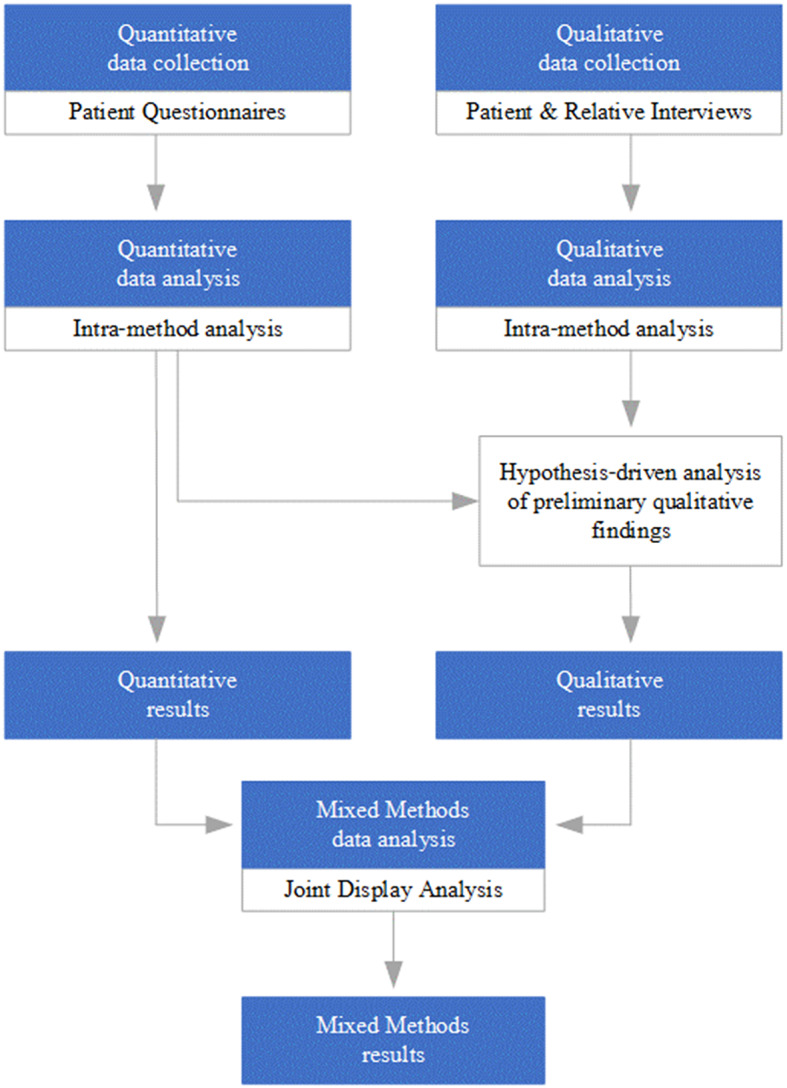
Methods: This study conducted in a German regional stroke network comprises a convergent quantitative-dominant, hypothesis-driven mixed methods design including 462 quantitative patient questionnaires combined with qualitative interviews with 28 patients and seven relatives. Quantitative associations were identified using Pearson's correlation analysis. Open coding was performed on interview transcripts before the quantitative results were used to further focus qualitative analysis. Joint display analysis was conducted to mix data strands. Cooperation with the Patient Council of the Department of Neurology ensured patient involvement in the study.
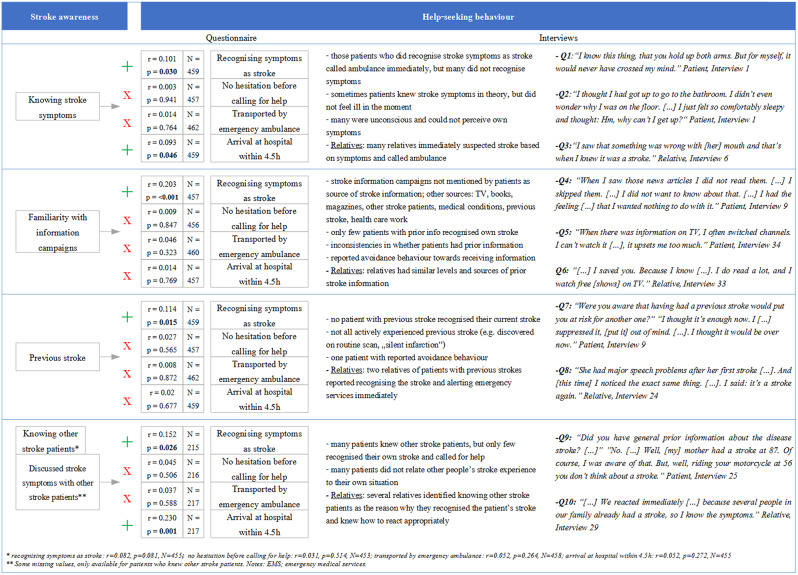
Results: Our hypothesis that stroke awareness would be associated with appropriate help-seeking behaviour at stroke symptom onset was partially supported by the quantitative data, i.e. showing associations between some dimensions of stroke awareness and appropriate help-seeking, but not others. For example, knowing stroke symptoms is correlated with recognising one's own symptoms as stroke (r = 0.101; p = 0.030*; N = 459) but not with no hesitation before calling help (r = 0.003; p = 0.941; N = 457). A previous stroke also makes it more likely to recognise one's own symptoms as stroke (r = 0.114; p = 0.015*; N = 459), but not to be transported by emergency ambulance (r = 0.08; p = 0.872; N = 462) or to arrive at the hospital on time (r = 0.02; p = 0.677; N = 459). Qualitative results showed concordance, discordance or provided potential explanations for quantitative findings. For example, qualitative data showed processes of denial on the part of patients and the important role of relatives in initiating appropriate help-seeking behaviour on patients' behalf.
Conclusions: Our study provides insights into the complexities of the decision-making process at stroke symptom onset. As our findings suggest processes of denial and inabilities to translate abstract disease knowledge into correct actions, we recommend to address relatives as potential saviours of loved ones, increased use of specific situational examples (e.g. lying on the bathroom floor) and the involvement of patient representatives in the preparation of informational resources and campaigns. Future research should include mixed methods research from one sample and more attention to potential reporting inconsistencies.
Keywords: Acute stroke; All clinical neurology; Help-seeking behaviour; Medical care; Mixed methods research; Qualitative research; Stroke awareness.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
