

Nomogram for predicting survival after first-line anti-PD-1-based immunotherapy in unresectable stage IV melanoma: a multicenter international study
- PMID: 39096893
- PMCID: PMC11345525
- DOI: 10.1016/j.esmoop.2024.103661
Nomogram for predicting survival after first-line anti-PD-1-based immunotherapy in unresectable stage IV melanoma: a multicenter international study
Abstract
Background: The introduction of anti-programmed cell death protein 1 (PD-1) immunotherapy has revolutionized the treatment landscape for melanoma, enhancing both response rates and survival outcomes in patients with advanced stages of the disease. Despite these remarkable advances, a noteworthy subset of patients (40%-60%) does not derive advantage from this therapeutic approach. This study aims to identify key predictive factors and create a user-friendly predictive nomogram for stage IV melanoma patients receiving first-line anti-PD-1-based immunotherapy, improving treatment decisions.
Materials and methods: In this retrospective study, we included patients with unresectable stage IV melanoma who received first-line treatment with either anti-PD-1 monotherapy or anti-PD-1 plus anti-cytotoxic T-lymphocyte associated protein 4 between 2014 and 2018. We documented clinicopathological features and blood markers upon therapy initiation. By employing the random survival forest model and backward variable selection of the Cox model, we identified variables associated with progression-free survival (PFS) after the first-line anti-PD-1-based treatment. We developed and validated a predictive nomogram for PFS utilizing the identified variables. We assessed calibration and discrimination performance metrics as part of the evaluation process.
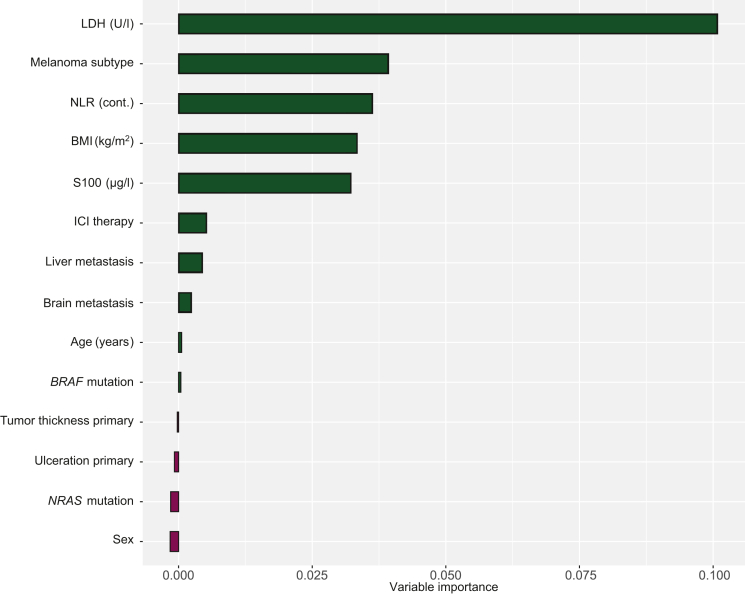
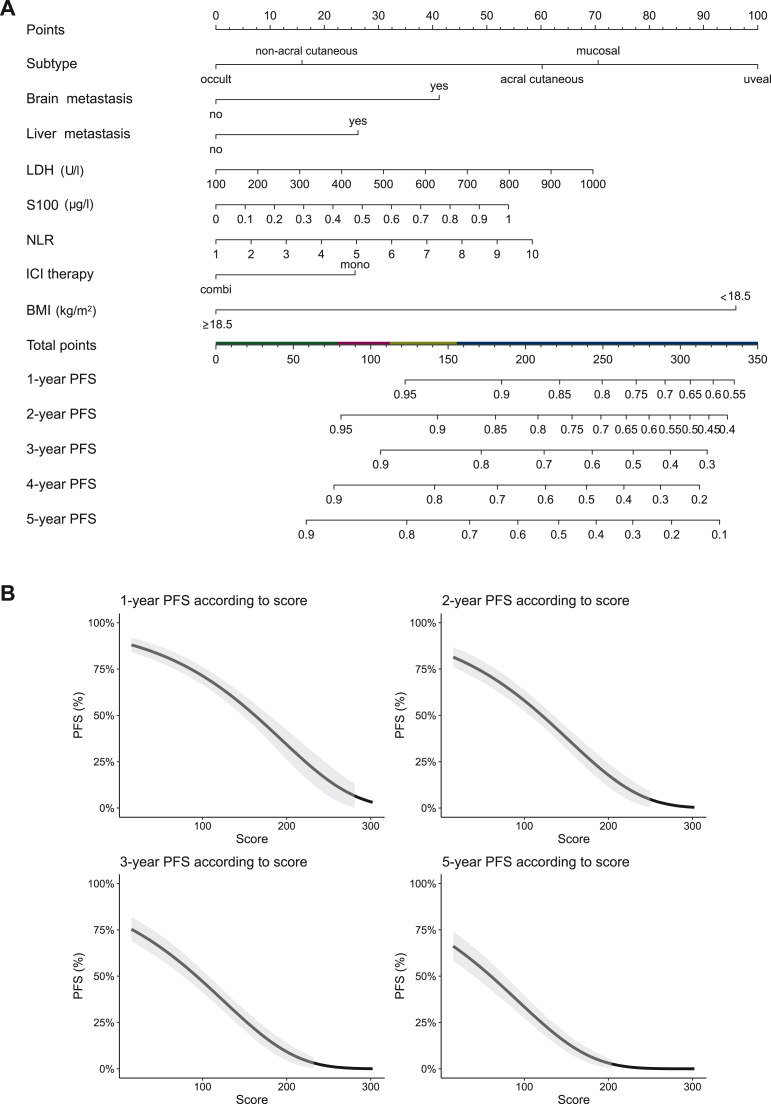
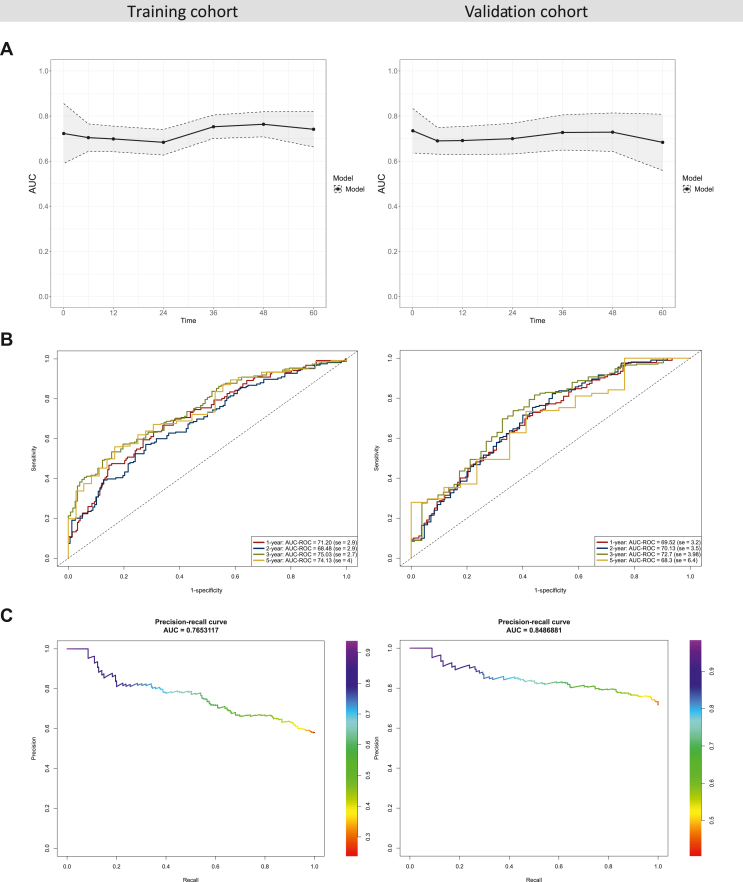
Results: The study involved 719 patients, divided into a training cohort of 405 (56%) patients and a validation cohort of 314 (44%) patients. We combined findings from the random survival forest and the Cox model to create a nomogram that incorporates the following factors: lactate dehydrogenase (LDH), S100, melanoma subtype, neutrophil-to-lymphocyte ratio (NLR), body mass index, type of immune checkpoint inhibitor, and presence of liver or brain metastasis. The resultant model had a C-index of 0.67 in the training cohort and 0.66 in the validation cohort. Performance remained in different patient subgroups. Calibration analysis revealed a favorable correlation between predicted and actual PFS rates.
Conclusions: We developed and validated a predictive nomogram for long-term PFS in patients with unresectable stage IV melanoma undergoing first-line anti-PD-1-based immunotherapy.
Keywords: anti-PD-1-based immunotherapy; biomarkers; immune checkpoint inhibition; nomogram; progression-free survival; stage IV melanoma.
Copyright © 2024 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures



References
-
- Atkins M.B., Julian C., Secrest M.H., Lee J., Abajo-Guijarro A.M., McKenna E. Real-world treatment patterns and overall survival in BRAF-mutant melanoma patients treated with immunotherapy or targeted therapy. Future Oncol. 2022;18(18):2233–2245. - PubMed
-
- Ascierto P.A., Mandalà M., Ferrucci P.F., et al. Sequencing of ipilimumab plus nivolumab and encorafenib plus binimetinib for untreated BRAF-mutated metastatic melanoma (SECOMBIT): a randomized, three-arm, open-label phase II trial. J Clin Oncol. 2023;41(2):212–221. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
