

Adrenal Suppression From Vamorolone and Prednisone in Duchenne Muscular Dystrophy: Results From the Phase 2b Clinical Trial
- PMID: 39097643
- PMCID: PMC11747748
- DOI: 10.1210/clinem/dgae521
Adrenal Suppression From Vamorolone and Prednisone in Duchenne Muscular Dystrophy: Results From the Phase 2b Clinical Trial
Abstract
Context: Vamorolone, a novel "dissociative" steroid, demonstrated similar efficacy in muscle function relative to prednisone 0.75 mg/kg/day but improved linear growth and bone turnover markers in a randomized trial of pediatric Duchenne muscular dystrophy (DMD).
Objectives: To determine the frequency of adrenal suppression (AS) induced by vamorolone and prednisone in pediatric DMD and to assess cortisol thresholds using a monoclonal antibody immunoassay.
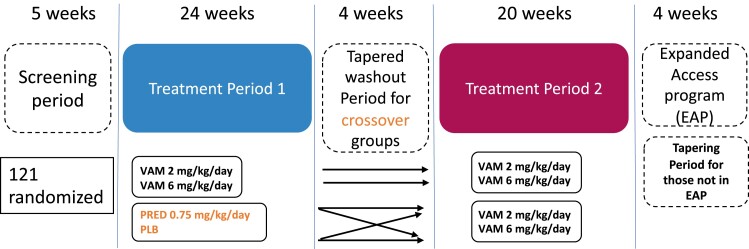
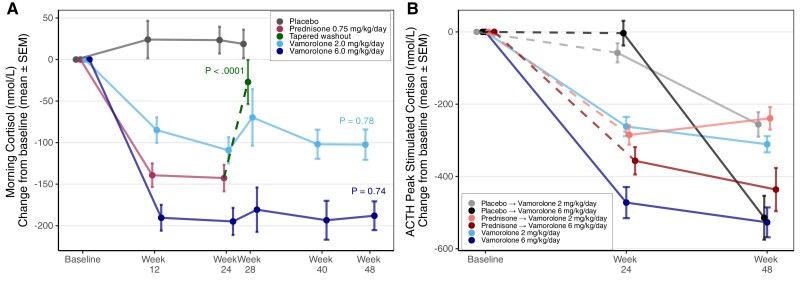
Methods: Post hoc analysis of cortisol levels was performed on data from a randomized, double-blind, placebo- and prednisone-controlled 24-week trial of vamorolone with a 24-week crossover extension. Morning and ACTH-stimulated cortisol levels were measured using the Elecsys II immunoassay, with AS defined as a stimulated cortisol of <500 nmol/L ("historical threshold") and <400 nmol/L ("revised threshold").
Results: Mean age at enrolment was 5.41 ± 0.86 years (n = 118). At week 24, the proportion of participants with AS using the historical and revised cortisol thresholds, respectively, were as follows: prednisone 0.75 mg/kg/day = 100% (25/25) and 92.0% (23/25); vamorolone 6 mg/kg/day = 95.2% (20/21) and 90.5% (19/21); vamorolone 2 mg/kg/day = 84.2% (16/19) and 47.5% (9/19); and placebo = 20.0% (4/20) and 0% (0/20). Morning and peak ACTH-stimulated cortisol were strongly correlated in steroid-treated boys (Spearman correlation week 48 = 0.83).
Conclusion: AS after vamorolone and prednisone was frequent and vamorolone-associated AS appeared dose-dependent. A lower stimulated cortisol threshold may be appropriate when using a monoclonal assay. We recommend hydrocortisone for glucocorticoid stress dosing in patients receiving vamorolone.
Keywords: Duchenne muscular dystrophy; adrenal insufficiency; adrenal suppression; prednisone; vamorolone.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures

References
-
- Bushby K, Finkel R, Birnkrant DJ, et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 2010;9(1):77‐93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
