

Clinical outcomes for immune checkpoint inhibitors plus chemotherapy in non-small-cell lung cancer patients with uncommon driver gene alterations
- PMID: 39097705
- PMCID: PMC11297614
- DOI: 10.1186/s12885-024-12748-y
Clinical outcomes for immune checkpoint inhibitors plus chemotherapy in non-small-cell lung cancer patients with uncommon driver gene alterations
Abstract
Background: Limited data exists on the efficacy of immune checkpoint inhibitor (ICI) combinations in non-small-cell lung cancer (NSCLC) with uncommon driver alterations in genes such as ERBB2, BRAF, RET, and MET. This study retrospectively assessed ICI-combination therapy outcomes in this molecular subset of NSCLC.
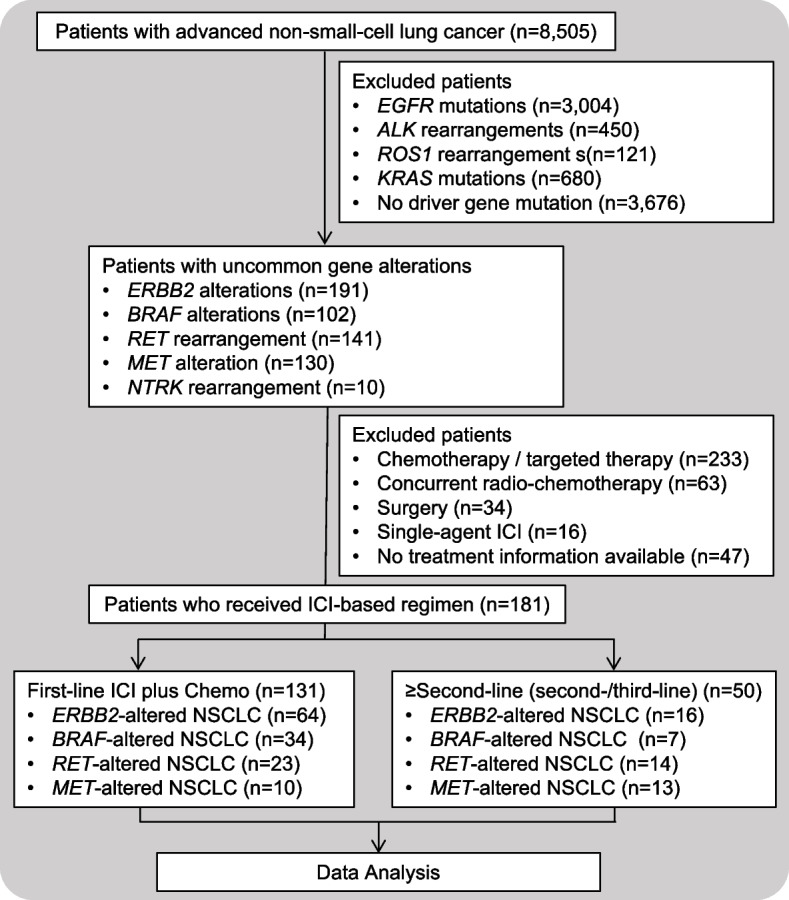
Methods: We retrospectively analyzed patients with advanced NSCLC confirmed with driver alterations in genes including ERBB2, BRAF, RET or MET, and received ICI combined with chemotherapy (ICI + chemo) and/or targeted therapy (ICI + chemo/TT) as first-line (1L) or second- or third-line (≥ 2L) treatment at Hunan Cancer Hospital between January 2018 and May 2024.
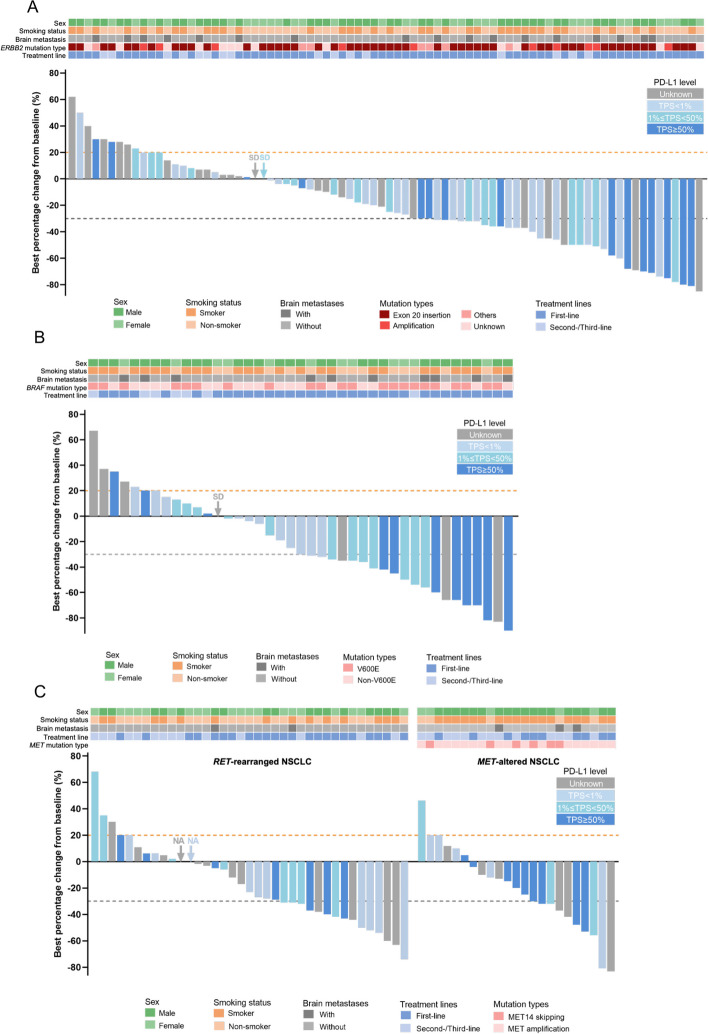
Results: Of the 181 patients included in the study, 131 patients received 1L-ICI + chemo (ERBB2, n = 64; BRAF, n = 34; RET, n = 23; and MET, n = 10), and 50 patients received ≥ 2L-ICI + chemo/TT (ERBB2, n = 16; BRAF, n = 7; RET, n = 14; MET, n = 13). The full cohort had an overall response rate (ORR) of 45.9% and disease control rate of 84.0%. Among patients who received 1L-ICI + chemo, ORR ranged between 51.6% and 60.0%, with the median progression-free survival (mPFS) and overall survival (mOS) of 8.2 and 21.0 months for those with ERBB2-altered tumors, 10.0 and 15.0 months for BRAF-altered tumors, 12.1 months and OS not reached for RET-altered tumors, and 6.2 and 28.0 months for MET-altered tumors, respectively. Additionally, ORR ranged between 14.3% and 30.8% for ≥ 2L-ICI + chemo/TT; mPFS and mOS were 5.4 and 16.2 months for patients with ERBB2-altered tumors, 2.7 and 5.0 months for BRAF-altered tumors, 6.2 and 14.3 months for RET-altered tumors, and 5.7 and 11.5 months for MET-altered tumors, respectively.
Conclusion: ICI-based combination therapies, regardless of treatment line, were effective in treating patients with advanced NSCLC harboring driver alterations in ERBB2, BRAF, RET, or MET. This suggests their potential as alternative treatment options in this patient population.
Keywords: BRAF; ERBB2; Immune checkpoint inhibitor; MET; RET.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Efficacy of chemotherapy plus immune checkpoint inhibitors in patients with non-small cell lung cancer who have rare oncogenic driver mutations: a retrospective analysis.BMC Cancer. 2024 Jul 15;24(1):842. doi: 10.1186/s12885-024-12554-6. BMC Cancer. 2024. PMID: 39009968 Free PMC article.
-
Efficacy of first-line immune checkpoint inhibitors in patients with advanced NSCLC with KRAS, MET, FGFR, RET, BRAF, and HER2 alterations.Thorac Cancer. 2022 Jun;13(11):1703-1711. doi: 10.1111/1759-7714.14448. Epub 2022 May 2. Thorac Cancer. 2022. PMID: 35491960 Free PMC article.
-
Efficacy and Safety of Anti-PD-1 Immunotherapy in Patients With Advanced NSCLC With BRAF, HER2, or MET Mutations or RET Translocation: GFPC 01-2018.J Thorac Oncol. 2020 Apr;15(4):628-636. doi: 10.1016/j.jtho.2019.12.129. Epub 2020 Jan 13. J Thorac Oncol. 2020. PMID: 31945494
-
Efficacy of immunotherapy in patients with oncogene-driven non-small-cell lung cancer: a systematic review and meta-analysis.Ther Adv Med Oncol. 2024 Feb 27;16:17588359231225036. doi: 10.1177/17588359231225036. eCollection 2024. Ther Adv Med Oncol. 2024. PMID: 38420602 Free PMC article. Review.
-
Clinical Outcomes of PD-1/PD-L1 Inhibitors Among Patients With Advanced or Metastatic Non-Small Cell Lung Cancer With BRAF, ERBB2/HER2, MET , or RET Alterations: A Systematic Literature Review.J Immunother. 2024 May 1;47(4):128-138. doi: 10.1097/CJI.0000000000000500. Epub 2023 Dec 19. J Immunother. 2024. PMID: 38112201 Free PMC article.
Cited by
-
Advances and Future Perspectives of HER2 Mutations in Non-Small Lung Cancer (NSCLC), Especially in China.Cancer Control. 2025 Jan-Dec;32:10732748251347572. doi: 10.1177/10732748251347572. Epub 2025 Jun 5. Cancer Control. 2025. PMID: 40472040 Free PMC article. Review.
-
Targeting the MET gene: unveiling therapeutic opportunities in immunotherapy within the tumor immune microenvironment of non-small cell lung cancer.Ther Adv Med Oncol. 2024 Oct 17;16:17588359241290733. doi: 10.1177/17588359241290733. eCollection 2024. Ther Adv Med Oncol. 2024. PMID: 39483139 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
