

Beyond tobacco: genomic disparities in lung cancer between smokers and never-smokers
- PMID: 39097719
- PMCID: PMC11297669
- DOI: 10.1186/s12885-024-12737-1
Beyond tobacco: genomic disparities in lung cancer between smokers and never-smokers
Abstract
Background: Tobacco use is one of the main risk factors for Lung Cancer (LC) development. However, about 10-20% of those diagnosed with the disease are never-smokers. For Non-Small Cell Lung Cancer (NSCLC) there are clear differences in both the clinical presentation and the tumor genomic profiles between smokers and never-smokers. For example, the Lung Adenocarcinoma (LUAD) histological subtype in never-smokers is predominately found in young women of European, North American, and Asian descent. While the clinical presentation and tumor genomic profiles of smokers have been widely examined, never-smokers are usually underrepresented, especially those of a Latin American (LA) background. In this work, we characterize, for the first time, the difference in the genomic profiles between smokers and never-smokers LC patients from Chile.
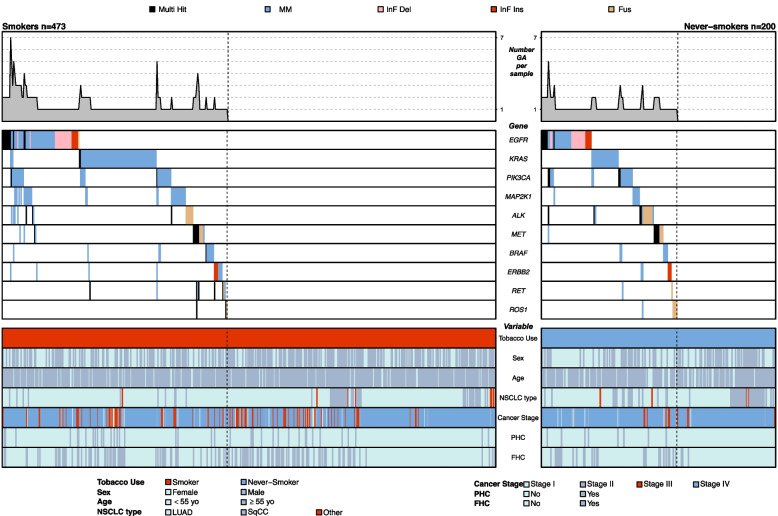
Methods: We conduct a comparison by smoking status in the frequencies of genomic alterations (GAs) including somatic mutations and structural variants (fusions) in a total of 10 clinically relevant genes, including the eight most common actionable genes for LC (EGFR, KRAS, ALK, MET, BRAF, RET, ERBB2, and ROS1) and two established driver genes for malignancies other than LC (PIK3CA and MAP2K1). Study participants were grouped as either smokers (current and former, n = 473) or never-smokers (n = 200) according to self-report tobacco use at enrollment.
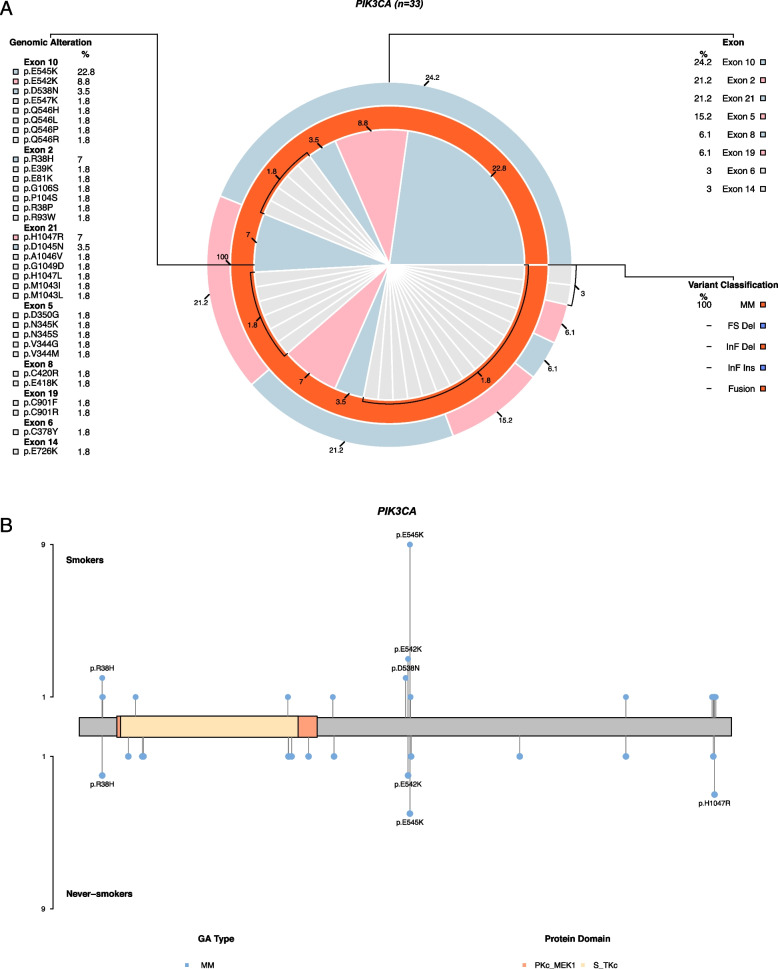
Results: Our findings indicate a higher overall GA frequency for never-smokers compared to smokers (58 vs. 45.7, p-value < 0.01) with the genes EGFR, KRAS, and PIK3CA displaying the highest prevalence while ERBB2, RET, and ROS1 the lowest. Never-smokers present higher frequencies in seven out of the 10 genes; however, smokers harbor a more complex genomic profile. The clearest differences between groups are seen for EGFR (15.6 vs. 21.5, p-value: < 0.01), PIK3CA (6.8 vs 9.5) and ALK (3.2 vs 7.5) in favor of never-smokers, and KRAS (16.3 vs. 11.5) and MAP2K1 (6.6 vs. 3.5) in favor of smokers. Alterations in these genes are comprised almost exclusively by somatic mutations in EGFR and mainly by fusions in ALK, and only by mutations in PIK3CA, KRAS and MAP2K1.
Conclusions: We found clear differences in the genomic landscape by smoking status in LUAD patients from Chile, with potential implications for clinical management in these limited-resource settings.
Keywords: Cancer disparities; Chilean; EGFR mutation; KRAS; Latin American populations; Lung Adenocarcinoma; MAP2K1; Tobacco consumption.
© 2024. The Author(s).
Conflict of interest statement
GS, AB, RA, RAC, MF, LR, DA, RL, JC and PP were Pfizer Chile employees. HF, EDN, DNN, GPB, MGA, CF, TFB, JF, MA, SC, OA, MLS, GR, CS, KM and SR received a grant and non-financial support for to perform this work for CEMP Pfizer Chile. Outside this work, HF discloses personal fees and non- financial support from Pfizer and BMS and non-financial support from AstraZeneca and Roche. RA declares honoraria for conferences, advisory boards, and educational activities from Roche, grants, and support for scientific research from Illumina, Pfizer, Roche & Thermo Fisher Scientific, and honoraria for conferences from Thermo Fisher Scientific, Janssen & Tecnofarma. The other authors declare that they have no competing interests. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures





References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
