

Progress and recognition of idiopathic intracranial hypertension: A narrative review
- PMID: 39097911
- PMCID: PMC11298205
- DOI: 10.1111/cns.14895
Progress and recognition of idiopathic intracranial hypertension: A narrative review
Abstract
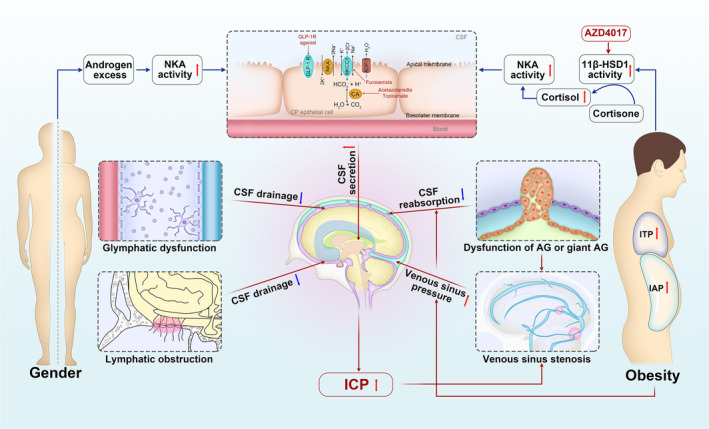
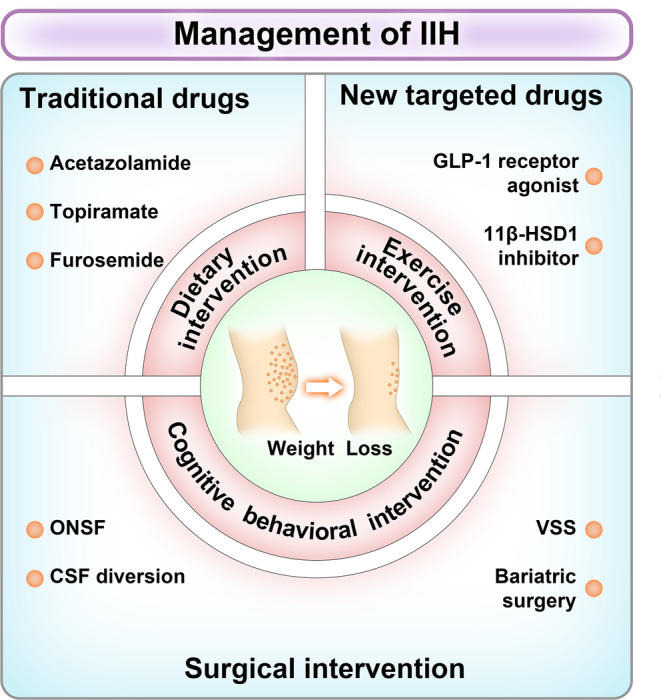
Background: Idiopathic intracranial hypertension (IIH) mainly affects obese young women, causing elevated intracranial pressure, headaches, and papilledema, risking vision loss and severe headaches. Despite weight loss as the primary treatment, the underlying mechanisms remain unclear. Recent research explores novel therapeutic targets.
Aims: This review aimed to provide a comprehensive understanding of IIH's pathophysiology and clinical features to inform pathogenesis and improve treatment strategies.
Methods: Recent publications on IIH were searched and summarized using PubMed, Web of Science, and MEDLINE.
Results: The review highlights potential pathomechanisms and therapeutic advances in IIH.
Conclusion: IIH incidence is rising, with growing evidence linking it to metabolic and hormonal disturbances. Early diagnosis and treatment remain challenging.
Keywords: 11β‐hydroxysteroid dehydrogenase type 1 (11β‐HSD1); glucagon‐like peptide‐1 (GLP‐1); idiopathic intracranial hypertension (IIH); intracranial pressure (ICP); venous sinus stenting (VSS).
© 2024 The Author(s). CNS Neuroscience & Therapeutics published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
