

Cytomegalovirus immunity in high-risk liver transplant recipients following preemptive antiviral therapy versus prophylaxis
- PMID: 39099206
- PMCID: PMC11457861
- DOI: 10.1172/jci.insight.180115
Cytomegalovirus immunity in high-risk liver transplant recipients following preemptive antiviral therapy versus prophylaxis
Abstract
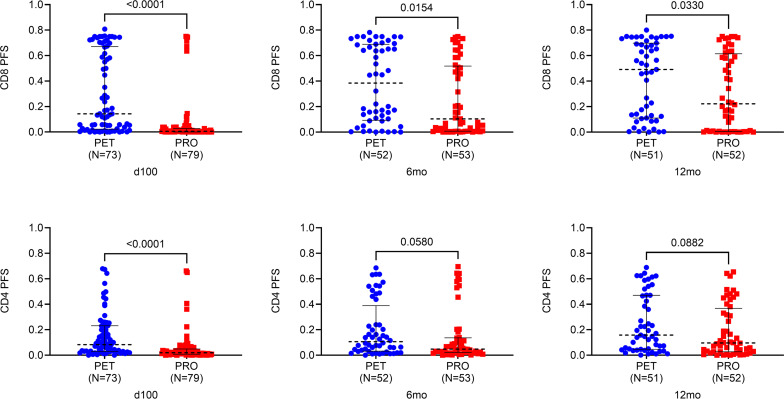
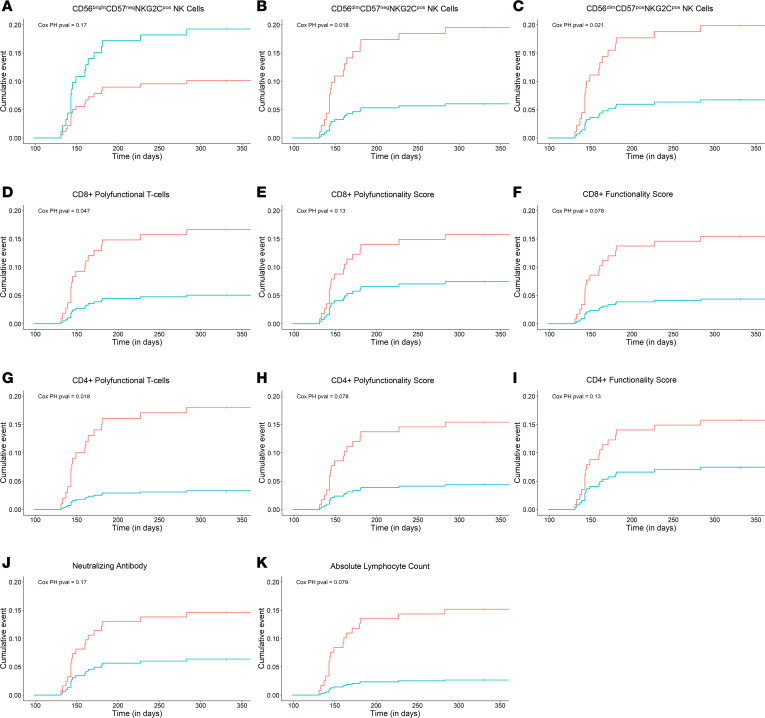
CMV-specific T cells, NK cells, and neutralizing antibodies (nAbs) were assessed in a randomized trial of CMV prevention with preemptive antiviral therapy (PET) versus prophylactic antiviral therapy (PRO) in donor-seropositive/recipient-seronegative (D+R-) liver transplant recipients (LTxR) at 100 days (end of intervention) and at 6 and 12 months after transplant. The PET group had significantly increased numbers of circulating polyfunctional T cells, NK cells, and nAbs compared with the PRO group at day 100, and several CMV immune parameters remained significantly higher by 12 months after transplant. Among PET recipients, preceding CMV viremia (vs. no preceding viremia) was associated with significantly higher levels of most CMV immune parameters at day 100. Higher numbers of CMV-specific polyfunctional T cells and NKG2C+ NK cells at day 100 were associated with a decreased incidence of CMV disease in multivariable Cox regression. The strongest associations with protection against CMV disease were with increased numbers of CMV-specific polyfunctional CD4+ T cells, CD3negCD56dimCD57negNKG2Cpos cells, and CD3negCD56dimCD57posNKG2Cpos NK cells. Our results suggest that PET is superior to PRO for CMV disease prevention by allowing low-level CMV replication and associated antigen exposure that is promptly controlled by antiviral therapy and facilitates enhanced CMV protective immunity in D+R- LTxR.
Keywords: Cellular immune response; Drug therapy; Infectious disease; Transplantation.
Figures







References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
