

Endoscope-Assisted Evacuation of an Acute Subdural Hematoma in an Elderly Patient With Refractory Nonconvulsive Status Epilepticus: An Illustrative Case
- PMID: 39099992
- PMCID: PMC11297714
- DOI: 10.7759/cureus.63817
Endoscope-Assisted Evacuation of an Acute Subdural Hematoma in an Elderly Patient With Refractory Nonconvulsive Status Epilepticus: An Illustrative Case
Abstract
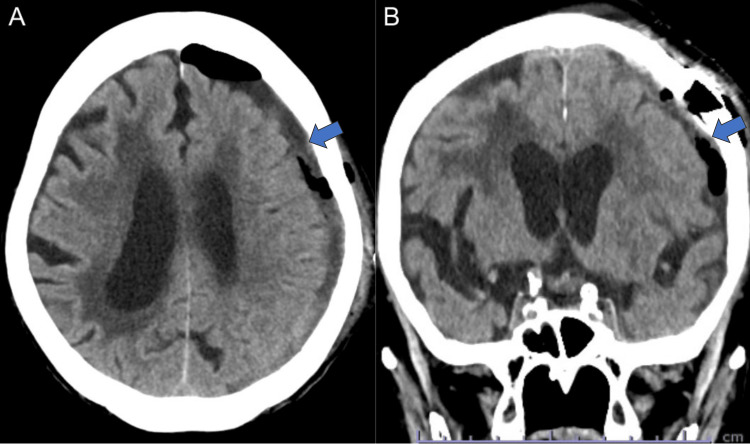
Traumatic brain injuries lead to post-traumatic seizures (PTS), with acute subdural hematomas (ASDH) posing a particularly elevated risk. The development of refractory nonconvulsive status epilepticus (NCSE) in such cases, especially in older patients, requires immediate and effective management. This case report highlights the improvement of refractory NCSE in an elderly patient with ASDH through endoscope-assisted evacuation. An 88-year-old woman was hospitalized for dysarthria and right hemiparesis 3 days after a fall. Computed tomography (CT) revealed a left hemispheric ASDH, 9 mm thick, along with minor traumatic subarachnoid bleeding in the interpeduncular cistern. The initial treatment was conservative, including the administration of lacosamide at 100 mg/day. However, her consciousness deteriorated 4 days after admission, and she experienced convulsions in the right face and arm on day 5. Although the convulsions stopped after the administration of diazepam 10 mg IV and her consciousness temporarily improved, it worsened again on day 6, leading to a diagnosis of NCSE on an electroencephalogram (EEG). Despite aggressive pharmacological interventions with fosphenytoin (750 mg initially followed by 262 mg/day) and phenobarbital (625 mg/day), the patient's cognitive state and EEG findings did not improve. Consequently, on the 13th day, she underwent an endoscopic procedure to remove the SDH, which alleviated her symptoms and ended the seizures. This case demonstrates that even the absence of a significant mass effect from ASDH can trigger NCSE, underscoring the necessity for swift diagnosis and consideration of surgical options when conventional treatment fails. Endoscope-assisted evacuation is a safe and effective treatment option, particularly in older patients.
Keywords: acute subdural hematomas; elderly; endoscopic assisted key hole surgery; non-convulsive status epilepticus; post-traumatic seizures.
Copyright © 2024, Arai et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




Similar articles
-
Endoscopic surgery for traumatic acute subdural hematoma.Case Rep Neurol. 2014 Jan 18;5(3):208-13. doi: 10.1159/000357367. eCollection 2013 Sep. Case Rep Neurol. 2014. PMID: 24659965 Free PMC article.
-
Effective management of nonconvulsive status epilepticus following cardiac surgery: a case report.Gen Thorac Cardiovasc Surg Cases. 2025 Jan 24;4(1):5. doi: 10.1186/s44215-025-00189-3. Gen Thorac Cardiovasc Surg Cases. 2025. PMID: 39856790 Free PMC article.
-
Nonconvulsive status epilepticus as sign of tumor recurrence.Epilepsy Behav Rep. 2023 Mar 23;22:100597. doi: 10.1016/j.ebr.2023.100597. eCollection 2023. Epilepsy Behav Rep. 2023. PMID: 37025369 Free PMC article.
-
Pharmacotherapy for Nonconvulsive Seizures and Nonconvulsive Status Epilepticus.Drugs. 2021 May;81(7):749-770. doi: 10.1007/s40265-021-01502-4. Epub 2021 Apr 8. Drugs. 2021. PMID: 33830480 Review.
-
Contralateral acute subdural hematoma following traumatic acute subdural hematoma evacuation.Neurol Med Chir (Tokyo). 2013;53(4):221-4. doi: 10.2176/nmc.53.221. Neurol Med Chir (Tokyo). 2013. PMID: 23615411 Review.
References
-
- Short- and long-term geriatric mortality after acute traumatic subdural hemorrhage. Benko MJ, Abdulla SG, Cuoco JA, et al. World Neurosurg. 2019;130:0–5. - PubMed
-
- Association of antithrombotic drug use with subdural hematoma risk. Gaist D, García Rodríguez LA, Hellfritzsch M, Poulsen FR, Halle B, Hallas J, Pottegård A. JAMA. 2017;317:836–846. - PubMed
-
- Acute subdural hematoma in patients on oral anticoagulant therapy: management and outcome. Won SY, Dubinski D, Bruder M, Cattani A, Seifert V, Konczalla J. Neurosurg Focus. 2017;43:0. - PubMed
-
- Prognosis of acute subdural hematoma in the elderly: a systematic review. Evans LR, Jones J, Lee HQ, et al. J Neurotrauma. 2019;36:517–522. - PubMed
Publication types
LinkOut - more resources
Full Text Sources