

Neuromyelitis Optica Spectrum Disorders Resembling Wernicke's Encephalopathy: A Case Report and Review of Literature
- PMID: 39100003
- PMCID: PMC11298258
- DOI: 10.7759/cureus.63920
Neuromyelitis Optica Spectrum Disorders Resembling Wernicke's Encephalopathy: A Case Report and Review of Literature
Abstract
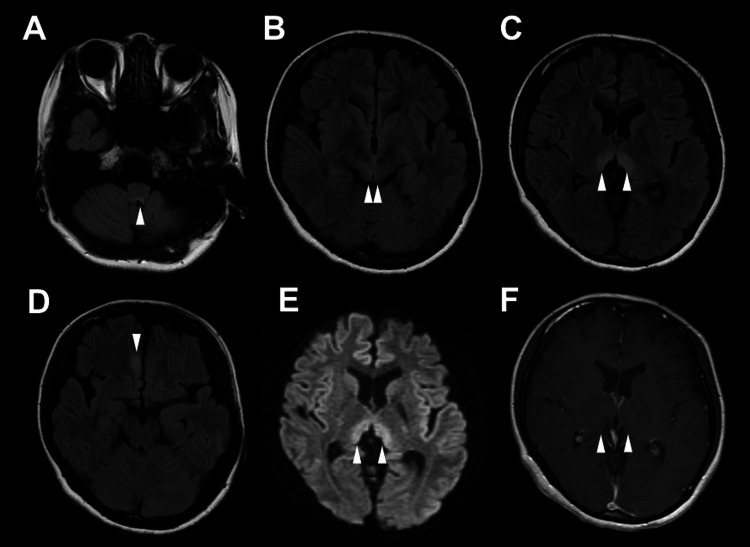
Both neuromyelitis optica spectrum disorder (NMOSD) and Wernicke's encephalopathy (WE) involve brain lesions. However, their treatments are quite different. In this report, we describe the case of a 29-year-old woman with NMOSD, who presented with clinical and imaging findings similar to those of WE. She was admitted to our hospital with a headache, vomiting, and loss of appetite for two weeks and diplopia for nine days. Magnetic resonance imaging revealed lesions in the area postrema, periaqueductal gray matter, thalamus, and right frontal lobe. Vitamin B1 supplementation was ineffective. The patient was diagnosed with NMOSD because serum aquaporin-4 antibody was detected after admission. Her symptoms improved with immunotherapy. The possibility of NMOSD should be considered in patients with suspected WE.
Keywords: brain diseases; encephalopathy; immunotherapy; neuromyelitis optica; radiology; wernicke encephalopathy.
Copyright © 2024, Saito et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Neuromyelitis Optica Spectrum Disorder Resembling Wernicke's Encephalopathy: A Case Report and Review of the Literature.Neurohospitalist. 2024 Apr;14(2):213-217. doi: 10.1177/19418744241228004. Epub 2024 Jan 16. Neurohospitalist. 2024. PMID: 38666289 Free PMC article.
-
Neuromyelitis Optica Spectrum Disorders Mimicking Wernicke's Encephalopathy: A Difficult Differential Diagnosis.Acta Neurol Taiwan. 2025 Jan 1;34(1):43-47. doi: 10.4103/ANT.ANT_112_0071. Epub 2025 Mar 28. Acta Neurol Taiwan. 2025. PMID: 40396803
-
Neuromyelitis Optica Spectrum Disorder.Cureus. 2023 Nov 2;15(11):e48168. doi: 10.7759/cureus.48168. eCollection 2023 Nov. Cureus. 2023. PMID: 38046734 Free PMC article.
-
Non-alcoholic Wernicke's Encephalopathy mimicking neuromyelitis optica spectrum disorder in a young woman: a case report and literature review.Acta Biomed. 2023 Jun 5;94(S1):e2023111. doi: 10.23750/abm.v94iS1.13879. Acta Biomed. 2023. PMID: 37272602 Review.
-
The pathogenesis and treatment of posterior reversible encephalopathy syndrome after neuromyelitis optica spectrum disorder: a case report and literature review.BMC Neurol. 2022 Dec 20;22(1):493. doi: 10.1186/s12883-022-02985-8. BMC Neurol. 2022. PMID: 36539740 Free PMC article. Review.
References
-
- Neuromyelitis optica spectrum disorder. Wingerchuk DM, Lucchinetti CF. N Engl J Med. 2022;387:631–639. - PubMed
-
- The spectrum of neuromyelitis optica. Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. Lancet Neurol. 2007;6:805–815. - PubMed
-
- Anti-aquaporin-4 antibody is involved in the pathogenesis of NMO: a study on antibody titre. Takahashi T, Fujihara K, Nakashima I, et al. Brain. 2007;130:1235–1243. - PubMed
-
- Neuromyelitis optica: evaluation of 871 attacks and 1,153 treatment courses. Kleiter I, Gahlen A, Borisow N, et al. Ann Neurol. 2016;79:206–216. - PubMed
Publication types
LinkOut - more resources
Full Text Sources