

Degenerative Mitral Regurgitation Outcomes in Asian Compared With European-American Institutions
- PMID: 39100700
- PMCID: PMC11291393
- DOI: 10.1016/j.jacasi.2024.03.003
Degenerative Mitral Regurgitation Outcomes in Asian Compared With European-American Institutions
Abstract
Background: Clinical outcome and interventional thresholds for degenerative mitral regurgitation (DMR) were developed in studies of patients at European and American institutions (EAIs), but little is known about patients at Asian institutions (AsIs).
Objectives: This study sought to contrast DMR presentation/management/outcomes of AsI patients vs EAI patients.
Methods: Patients with DMR due to flail leaflet from Hong Kong and Singapore (AsI cohort, n = 737) were compared with EAI patients (n = 682) enrolled in the MIDA (Mitral regurgitation International Database) registry with similar eligibility criteria.
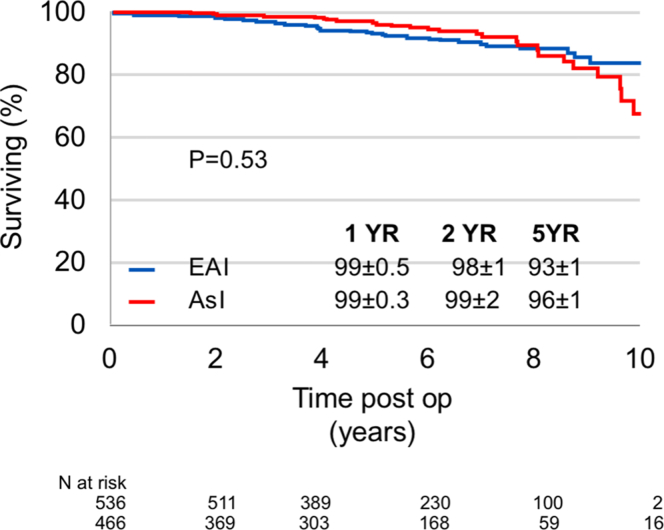
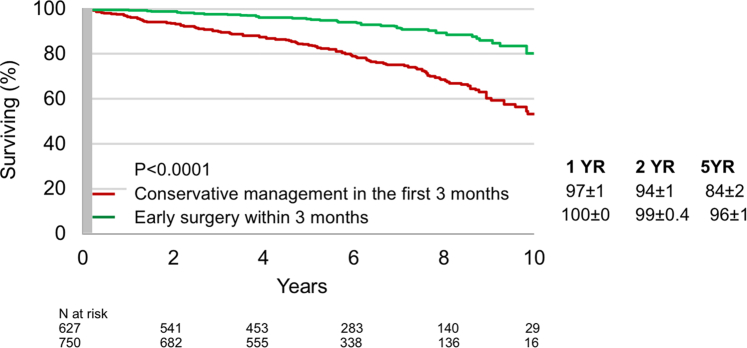
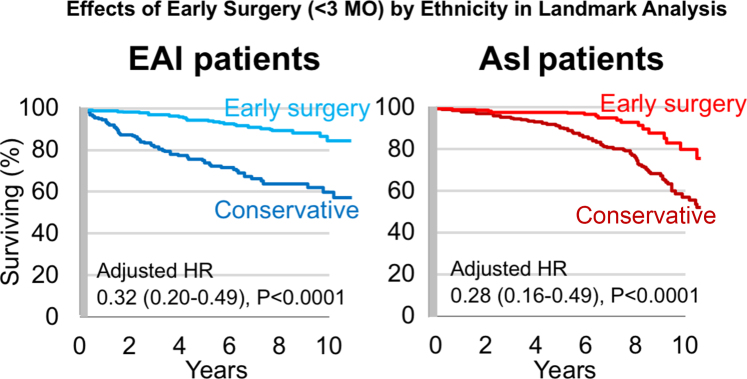
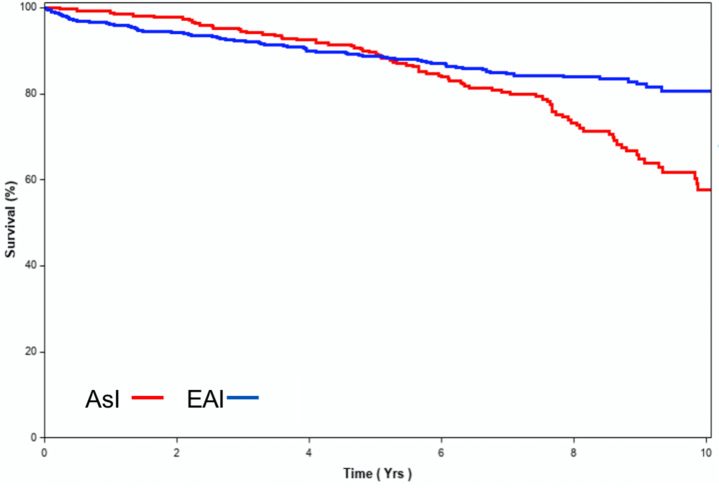
Results: AsI patients presented similar DMR lesion/consequences vs EAI patients, but they were younger, with fewer symptoms (74% vs 44% Class I), more sinus rhythm (83% vs 69%), and lower EuroSCORE II (European System for Cardiac Operative Risk Evaluation II) (0.9 ± 0.5 vs 1.4 ± 1.5; all P < 0.0001). Imaging showed smaller absolute left atrial/ventricular dimensions in AsI patients, belying cardiac dilatation with larger body surface area-indexed diameters (all P < 0.01). Surgical/interventional mitral repair was similarly predominant (90% vs 91%; P = 0.47), and early repair was similarly beneficial (for AsI patients, adjusted HR: 0.28; 95% CI: 0.16-0.49; for EAI patients, HR: 0.32; 95% CI: 0.20-0.49; both P < 0.0001). However, AsI patients underwent fewer interventions (55% ± 2% vs 77% ± 2% at 1 year; P < 0.0001) and incurred excess mortality (adjusted HR: 1.60 [95% CI: 1.13-2.27] vs EAI patients; P = 0.008) at long-term postdiagnosis. Propensity score matching (434 patient pairs), which balanced all clinical characteristics, confirmed that there was undertreatment and excess mortality in the long term in AsI patients with DMR (P < 0.0001).
Conclusions: Imaging may underestimate volume overload in AsI patients due to smaller cardiac cavities related to smaller body size compared with EAI patients with similar mitral lesions and DMR severity. AsI patients enjoy similar mitral repair predominance and early intervention benefits but undergo fewer mitral interventions than EAI patients and incur subsequent excess mortality, suggesting the need to account for imaging and cultural specificity to improve DMR outcomes worldwide.
Keywords: degenerative mitral regurgitation; ethnicity; mitral surgery; outcome.
© 2024 The Authors.
Conflict of interest statement
Dr Enriquez-Sarano has received personal fees from Edwards LLC, ChemImage Inc, and CryoLife Inc, outside the submitted work. Dr Ding has received personal fees from GE Healthcare; and nonfinancial support from Phillips Healthcare, outside the submitted work. Dr Lee has received grant support from Abbott, outside the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Ling L.H., Enriquez-Sarano M., Seward J.B., et al. Clinical outcome of mitral regurgitation due to flail leaflet. N Engl J Med. 1996;335:1417–1423. - PubMed
-
- Grigioni F., Tribouilloy C., Avierinos J.F., et al. Outcomes in mitral regurgitation due to flail leaflets a multicenter European study. J Am Coll Cardiol Img. 2008;1:133–141. - PubMed
-
- Dziadzko V., Dziadzko M., Medina-Inojosa J.R., et al. Causes and mechanisms of isolated mitral regurgitation in the community: clinical context and outcome. Eur Heart J. 2019;40:2194–2202. - PubMed
-
- Iung B., Delgado V., Rosenhek R., et al. Contemporary presentation and management of valvular heart disease: the EURObservational Research Programme Valvular Heart Disease II Survey. Circulation. 2019;140:1156–1169. - PubMed
LinkOut - more resources
Full Text Sources
