

Blood Hemoglobin Concentrations and the Incidence of Lower Extremity Peripheral Arterial Disease in Patients Undergoing Hemodialysis: 10-Year Outcomes of the Q-Cohort Study
- PMID: 39101503
- PMCID: PMC11964019
- DOI: 10.1161/JAHA.123.033853
Blood Hemoglobin Concentrations and the Incidence of Lower Extremity Peripheral Arterial Disease in Patients Undergoing Hemodialysis: 10-Year Outcomes of the Q-Cohort Study
Abstract
Background: Lower extremity peripheral arterial disease is a potentially lethal cardiovascular complication in patients undergoing hemodialysis. Anemia is a risk factor for cardiovascular disease among the hemodialysis population. However, whether blood hemoglobin concentration is associated with the risk of peripheral arterial disease progression in this population remains undetermined.
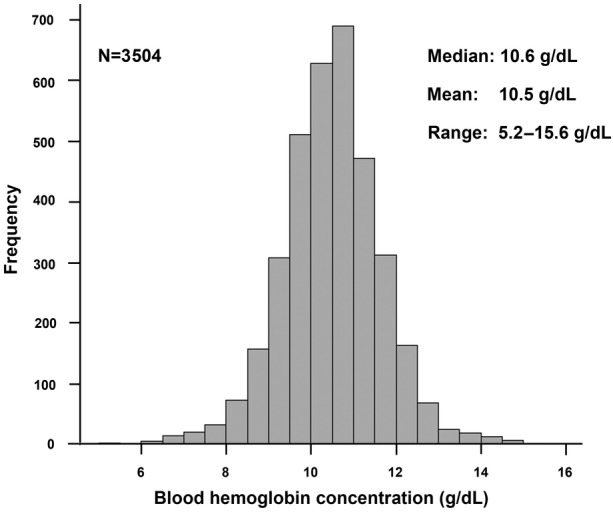
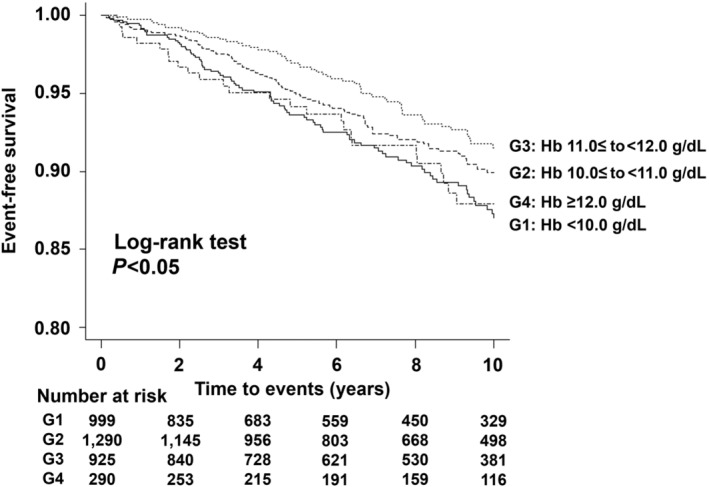
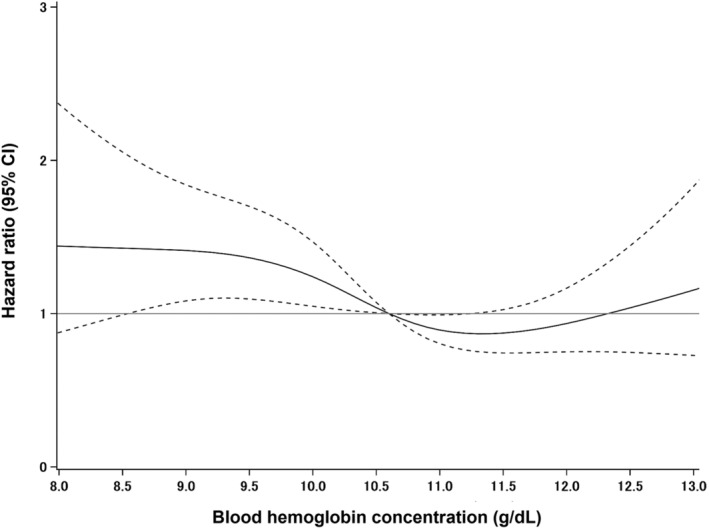
Methods and results: This is an extension of a 4-year multicenter, prospective, observational cohort study to 10 years. A total of 3504 Japanese patients undergoing maintenance hemodialysis were recruited between 2006 and 2007. The primary exposure was blood hemoglobin concentration at baseline. The main outcome was the first-ever incidence of major adverse limb events (MALE), composed of endovascular treatment, bypass surgery, and amputation. Multivariable-adjusted Cox proportional hazards model, Fine-Gray subdistribution hazards model, restricted cubic spline analysis, and restricted mean survival time analysis were used to determine the association of blood hemoglobin concentration with the incidence of MALE. During a median follow-up of 8.0 years, 257 patients experienced MALE. A Cox proportional hazards model showed that the risk of MALE in patients with blood hemoglobin concentrations <10.0 g/dL was significantly higher than in patients with concentrations of 11.0 to 11.9 g/dL, even after adjusting for confounding factors. In contrast, elevated hemoglobin concentration (≥12.0 g/dL) was not significantly associated with increased risk of MALE. Similar associations were observed when the Fine-Gray subdistribution regression model was used by setting all-cause mortality as the competing risk.
Conclusions: A low blood hemoglobin concentration is an independent risk factor for peripheral arterial disease progression in patients undergoing maintenance hemodialysis.
Keywords: anemia; blood hemoglobin concentration; hemodialysis; major adverse limb events; peripheral arterial disease.
Figures
Similar articles
-
Association of Anemia and Transfusion with Major Adverse Cardiac Events and Major Adverse Limb Events in Patients Undergoing Open Infrainguinal Bypass.Ann Vasc Surg. 2025 Feb;111:25-38. doi: 10.1016/j.avsg.2024.10.007. Epub 2024 Oct 20. Ann Vasc Surg. 2025. PMID: 39437935
-
Indoxyl Sulfate and Incident Peripheral Artery Disease in Hemodialysis Patients.Toxins (Basel). 2020 Nov 2;12(11):696. doi: 10.3390/toxins12110696. Toxins (Basel). 2020. PMID: 33147880 Free PMC article.
-
High hemoglobin A1c associated with increased adverse limb events in peripheral arterial disease patients undergoing revascularization.J Vasc Surg. 2018 Jan;67(1):217-228.e1. doi: 10.1016/j.jvs.2017.06.101. Epub 2017 Aug 31. J Vasc Surg. 2018. PMID: 28844470 Free PMC article.
-
Mortality rates and walking ability transition after lower limb major amputation in hemodialysis patients.J Vasc Surg. 2016 Oct;64(4):1018-25. doi: 10.1016/j.jvs.2016.03.452. Epub 2016 May 14. J Vasc Surg. 2016. PMID: 27189770
-
The prognosis of patients on hemodialysis with foot lesions.J Vasc Surg. 2013 Nov;58(5):1291-9. doi: 10.1016/j.jvs.2013.05.027. Epub 2013 Jun 27. J Vasc Surg. 2013. PMID: 23810259
References
-
- Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–1340. doi: 10.1016/S0140-6736(13)61249-0 - DOI - PubMed
-
- Armstrong EJ, Chen DC, Westin GG, Singh S, McCoach CE, Bang H, Yeo KK, Anderson D, Amsterdam EA, Laird JR. Adherence to guideline‐recommended therapy is associated with decreased major adverse cardiovascular events and major adverse limb events among patients with peripheral arterial disease. J Am Heart Assoc. 2014;3:e000697. doi: 10.1161/JAHA.113.000697 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
