

Angiography-derived physiological patterns of coronary artery disease: implications with post-stenting physiology and long-term clinical outcomes
- PMID: 39102003
- PMCID: PMC11579185
- DOI: 10.1007/s00392-024-02500-8
Angiography-derived physiological patterns of coronary artery disease: implications with post-stenting physiology and long-term clinical outcomes
Abstract
Background: Physiological patterns of coronary artery disease (CAD) have emerged as potential determinants of functional results of percutaneous coronary interventions (PCI) and of vessel-oriented clinical outcomes (VOCE).
Objectives: In this study, we evaluated the impact of angiography-derived physiological patterns of CAD on post-PCI functional results and long-term clinical outcomes.
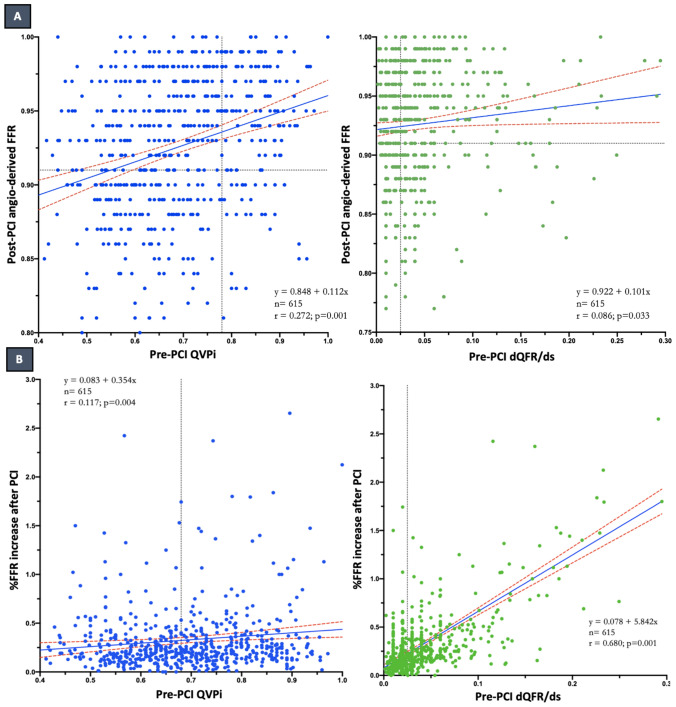
Methods: Pre-PCI angiography-derived fractional flow reserve (FFR) virtual pullbacks were quantitatively interpreted and used to determine the physiological patterns of CAD. Suboptimal post-PCI physiology was defined as an angiography-derived FFR value ≤ 0.91. The primary endpoint was the occurrence of VOCE at the longest available follow-up.
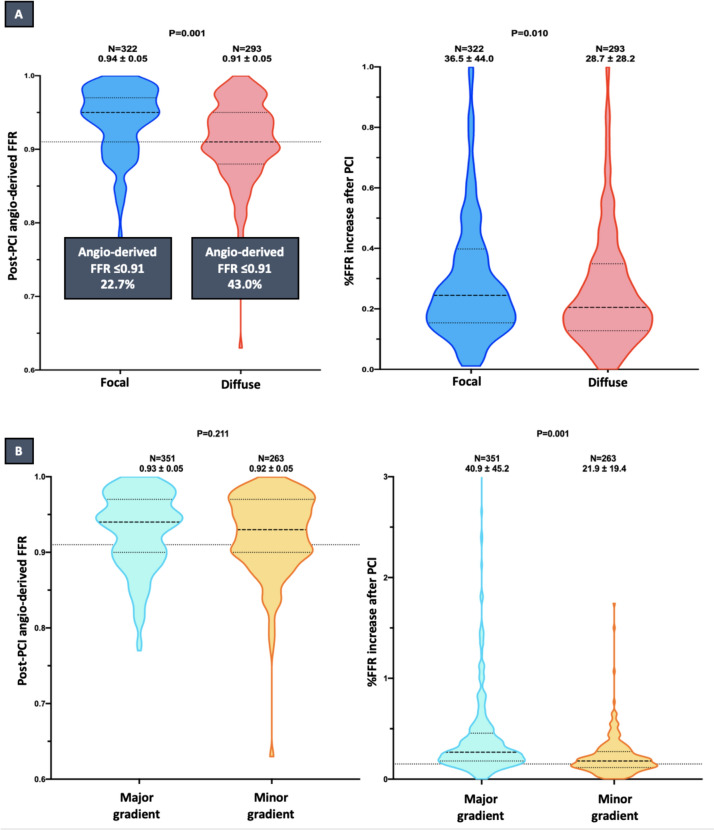
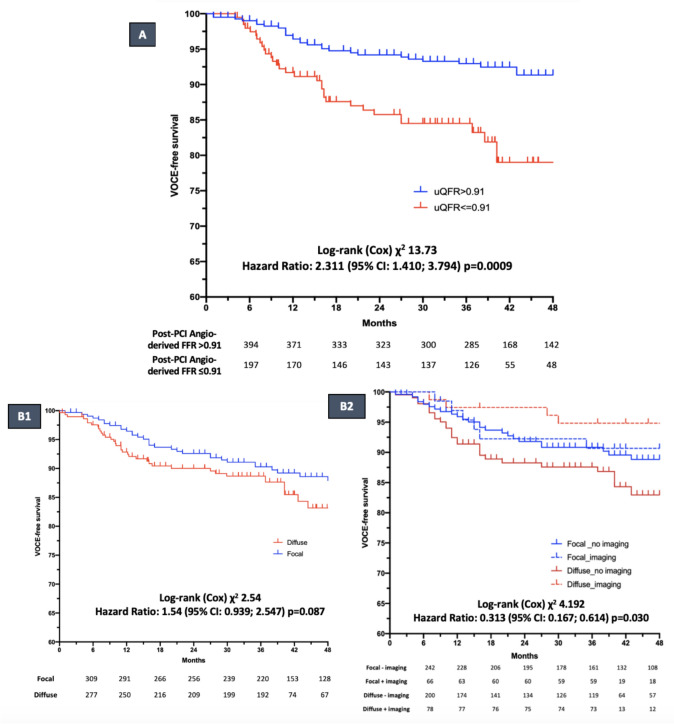
Results: Six hundred fifteen lesions from 516 patients were stratified into predominantly focal (n = 322, 52.3%) and predominantly diffuse (n = 293, 47.7%). Diffuse pattern of CAD was associated with lower post-PCI angiography-derived FFR values (0.91 ± 0.05 vs. 0.94 ± 0.05; p = 0.001) and larger rate of suboptimal post-PCI physiology (43.0 vs. 22.7%; p = 0.001), as compared to focal CAD. At the median follow-up time of 37 months (33-58), post-PCI suboptimal physiology was related to a higher risk of VOCE (16.2% vs. 7.6%; HR: 2.311; 95% CI 1.410-3.794; p = 0.0009), while no significant difference was noted according to baseline physiological pattern. In diffuse disease, the use of intracoronary imaging was associated with a lower incidence of long-term VOCE (5.1% vs 14.8%; HR: 0.313, 95% CI 0.167-0.614, p = 0.030).
Conclusions: Suboptimal post-PCI physiology is observed more often in diffusely diseased arteries and it is associated with higher risk of VOCE at follow-up. The use of intravascular imaging might improve clinical outcomes in the setting of diffuse CAD.
Keywords: Angiography-derived physiology; Intracoronary imaging; Percutaneous coronary intervention; Physiological pattern of coronary disease; Quantitative flow ratio.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: ST is the co-founder of Pulse Medical, reports research grants and consultancy from Pulse Medical. WW reports grants and consulting fees from MicroPort, outside the submitted work, and medical advisor of Corrib Core Laboratory and Rede Optimus, co-founder of Argonauts, an innovation facilitator. RS reports speaker fees from Abbott Vascular and research grant from Philips and Abbott. FR reports research grant from Philips and Abbott. All other authors report no competing interests.
Figures
References
-
- Fihn SD, Gardin JM, Abrams J, Berra K, Blankenship JC, Dallas AP, Douglas PS, Foody JM, Gerber TC, Hinderliter AL, King SB 3rd, Kligfield PD, Krumholz HM, Kwong RY, Lim MJ, Linderbaum JA, Mack MJ, Munger MA, Prager RL, Sabik JF, Shaw LJ, Sikkema JD, Smith CR Jr, Smith SC Jr, Spertus JA, Williams SV, Anderson JL, American College of Cardiology Foundation/American Heart Association Task Force (2012) ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 126:354–471 - PubMed
-
- Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet JP, Falk V, Head SJ, Jüni P, Kastrati A, Koller A, Kristensen SD, Niebauer J, Richter DJ, Seferović PM, Sibbing D, Stefanini GG, Windecker S, Yadav R, Zembala MO (2018) ESC/EACTS guidelines on myocardial revascularization. EuroIntervention 2019(14):1435–1534 - PubMed
-
- Johnson NP, Tóth GG, Lai D, Zhu H, Açar G, Agostoni P, Appelman Y, Arslan F, Barbato E, Chen SL, Di Serafino L, Domínguez-Franco AJ, Dupouy P, Esen AM, Esen OB, Hamilos M, Iwasaki K, Jensen LO, Jiménez-Navarro MF, Katritsis DG, Kocaman SA, Koo BK, López-Palop R, Lorin JD, Miller LH, Muller O, Nam CW, Oud N, Puymirat E, Rieber J, Rioufol G, Rodés-Cabau J, Sedlis SP, Takeishi Y, Tonino PA, Van Belle E, Verna E, Werner GS, Fearon WF, Pijls NH, De Bruyne B, Gould KL (2014) Prognostic value of fractional flow reserve: linking physiologic severity to clinical outcomes. J Am Coll Cardiol 64:1641–1654 - PubMed
-
- Rimac G, Fearon WF, De Bruyne B, Ikeno F, Matsuo H, Piroth Z, Costerousse O, Bertrand OF (2017) Clinical value of post-percutaneous coronary intervention fractional flow reserve value: a systematic review and meta-analysis. Am Heart J 183:1–9 - PubMed
-
- Collet C, Collison D, Mizukami T, McCartney P, Sonck J, Ford T, Munhoz D, Berry C, De Bruyne B, Oldroyd K (2022) Differential Improvement in Angina and health-related quality of life after PCI in focal and diffuse coronary artery disease JACC. Cardiovasc Interv 15:2506–2518 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
