Risk of Perinatal and Maternal Morbidity and Mortality Among Pregnant Women With Epilepsy
- PMID: 39102246
- PMCID: PMC11385047
- DOI: 10.1001/jamaneurol.2024.2375
Risk of Perinatal and Maternal Morbidity and Mortality Among Pregnant Women With Epilepsy
Abstract
Importance: Maternal epilepsy is associated with adverse pregnancy and neonatal outcomes. A better understanding of this condition and the associated risk of mortality and morbidity at the time of delivery could help reduce adverse outcomes.
Objective: To determine the risk of severe maternal and perinatal morbidity and mortality among women with epilepsy.
Design, setting, participants: This prospective population-based register study in Denmark, Finland, Iceland, Norway, and Sweden took place between January 1, 1996, and December 31, 2017. Data analysis was performed from August 2022 to November 2023. Participants included all singleton births at 22 weeks' gestation or longer. Births with missing or invalid information on birth weight or gestational length were excluded. The study team identified 4 511 267 deliveries, of which 4 475 984 were to women without epilepsy and 35 283 to mothers with epilepsy.
Exposure: Maternal epilepsy diagnosis recorded before childbirth. Prenatal exposure to antiseizure medication (ASM), defined as any maternal prescription fills from conception to childbirth, was also examined.
Main outcomes and measures: Composite severe maternal morbidity and mortality occurring in pregnancy or within 42 days postpartum and composite severe neonatal morbidity (eg, neonatal convulsions) and perinatal mortality (ie, stillbirths and deaths) during the first 28 days of life. Multivariable generalized estimating equations with logit-link were used to obtain adjusted odds ratios (aORs) and 95% CIs.
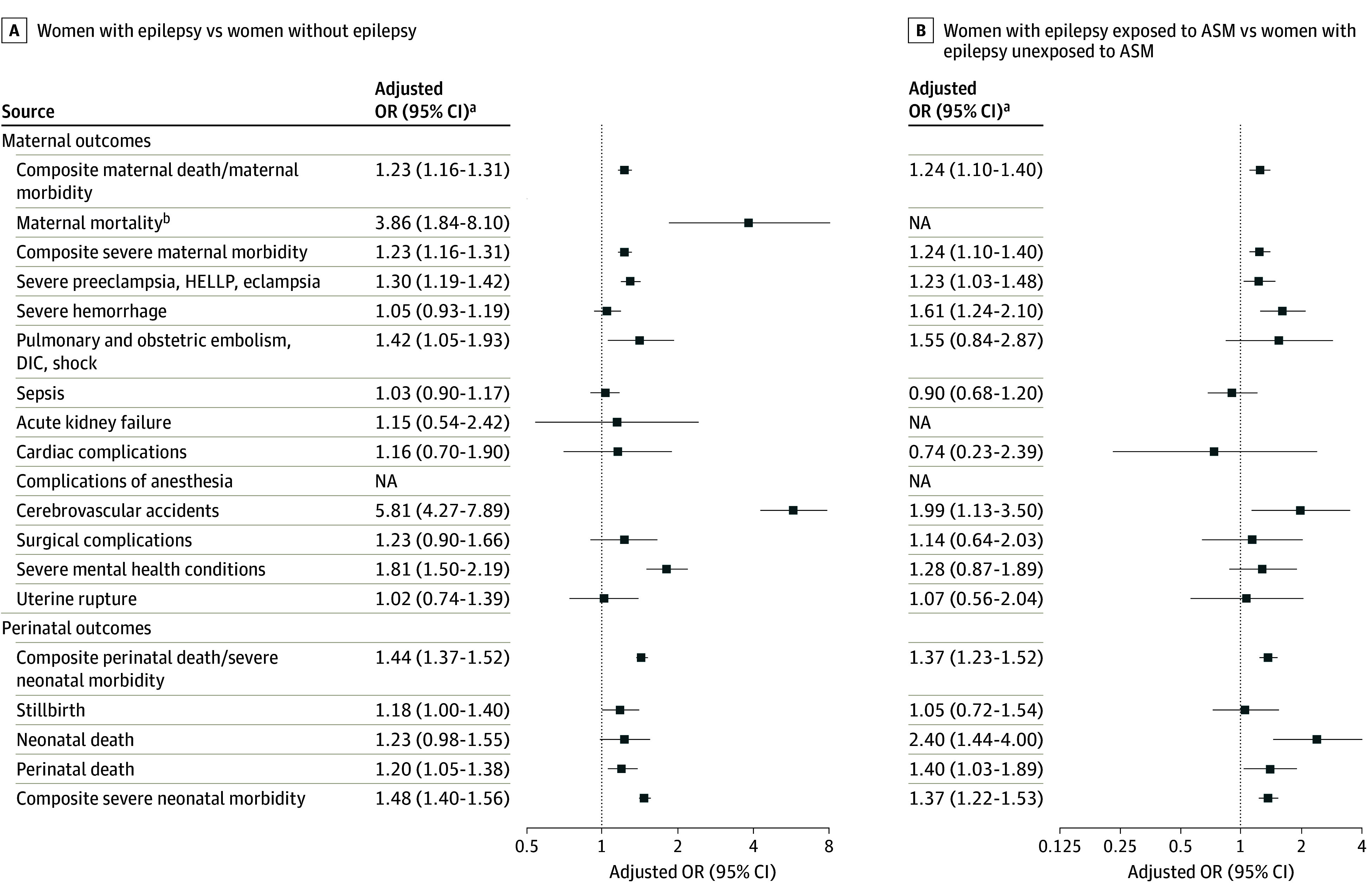
Results: The mean (SD) age at delivery for women in the epilepsy cohort was 29.9 (5.3) years. The rate of composite severe maternal morbidity and mortality was also higher in women with epilepsy compared with those without epilepsy (36.9 vs 25.4 per 1000 deliveries). Women with epilepsy also had a significantly higher risk of death (0.23 deaths per 1000 deliveries) compared with women without epilepsy (0.05 deaths per 1000 deliveries) with an aOR of 3.86 (95% CI, 1.48-8.10). In particular, maternal epilepsy was associated with increased odds of severe preeclampsia, embolism, disseminated intravascular coagulation or shock, cerebrovascular events, and severe mental health conditions. Fetuses and infants of women with epilepsy were at elevated odds of mortality (aOR, 1.20; 95% CI, 1.05-1.38) and severe neonatal morbidity (aOR, 1.48; 95% CI, 1.40-1.56). In analyses restricted to women with epilepsy, women exposed to ASM compared with those unexposed had higher odds of severe maternal morbidity (aOR ,1.24; 95% CI, 1.10-1.48) and their neonates had an increased odd of mortality and severe morbidity (aOR, 1.37; 95% CI, 1.23-1.52).
Conclusion and relevance: This multinational study shows that women with epilepsy were at considerably higher risk of severe maternal and perinatal outcomes and increased risk of death during pregnancy and postpartum. Maternal epilepsy and maternal use of ASM were associated with increased maternal morbidity and perinatal mortality and morbidity.
Conflict of interest statement
Figures