

Sex-difference of multifactorial intervention on cardiovascular and mortality risk in DKD: post-hoc analysis of a randomised clinical trial
- PMID: 39103870
- PMCID: PMC11299289
- DOI: 10.1186/s12933-024-02371-3
Sex-difference of multifactorial intervention on cardiovascular and mortality risk in DKD: post-hoc analysis of a randomised clinical trial
Abstract
Objective: Women with type 2 diabetes experience higher cardiovascular and mortality risk than men possibly because of a sub-optimal cardio-protective treatment. We evaluated whether an intensive multifactorial therapy (MT) produces similar protective effect on development of adverse outcomes in women and men.
Research design and methods: Nephropathy in Diabetes type 2 study is an open-label cluster randomized trial comparing the effect of Usual Care (UC) or MT of main cardiovascular risk factors (blood pressure < 130/80 mmHg, HbA1c < 7%, LDL < 100 mg/dL, and total cholesterol < 175 mg/dL) on cardiovascular and mortality risk in patients with type 2 diabetes. In this post-hoc analysis, we stratified patients by sex to compare the occurrence of MACEs (primary endpoint) and all-cause death (secondary endpoint) between women (104 MT and 105 UC) and men (103 MT and 83 UC).
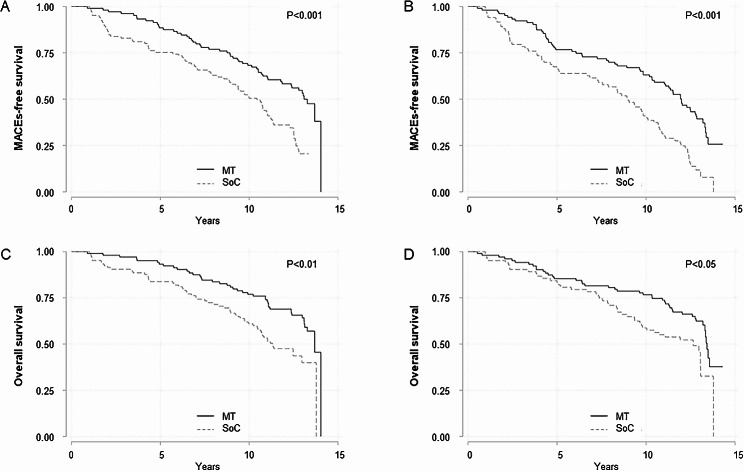
Results: Achievement of therapeutic goals was similar by sex, with 44% and 47% of women and men in MT achieving at least 3 targets vs. 16% and 20% of women and men in UC. During a median follow-up of 13.0 years, we recorded 262 MACE (48.5% in women) and 189 deaths (53.6% in women). Compared to the UC group, the risk of MACE in the MT group was reduced by 52% in women and by 44% in men (P = 0.11). Conversely, the reduction in mortality risk by MT was greater in women (44% versus 12%, P = 0.019).
Conclusions: MT similarly reduces the risk of MACEs in either sex. This therapeutic approach is associated with a survival advantage in women as compared with men and it may represent an important rationale to motivate physicians in overcoming their therapeutic inertia often encountered in female patients as well as to encourage patients of both sexes at improving their adherence to multidrug therapy.
© 2024. The Author(s).
Conflict of interest statement
Roberto Minutolo has been member of Advisory Boards for Astellas, and invited speaker at meetings supported by Amgen, Astellas, Vifor Pharma, Bayer, Astrazeneca. Luca De Nicola has received fees for scientific consultation and/or lectures by Astellas, AstraZeneca, Bayer, Novo. Ferdinando Carlo Sasso has been member of Advisory Boards for Boehringer and for Ely-Lilly and has received fees for scientific consultation and/or lectures by Jansen, Roche Diagnostics, Novo Nordisk, Sanofi, MSD, Astrazeneca. Vittorio Simeon, Paolo Chiodini, Raffaele Galiero, Luca Rinaldi, Raffaele Marfella, Celestino Sardu, have no conflict of interest to disclose.
Figures
References
-
- Prospective Studies Collaboration, Asia Pacific Cohort Studies Collaboration. Sex-specific relevance of diabetes to occlusive vascular and other mortality: a collaborative meta-analysis of individual data from 980 793 adults from 68 prospective studies. Lancet Diabetes Endocrinol. 2018;6(7):538–46. 10.1016/S2213-8587(18)30079-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
