

Brain modulation after exergaming training in advanced forms of Parkinson's disease: a randomized controlled study
- PMID: 39103924
- PMCID: PMC11299301
- DOI: 10.1186/s12984-024-01430-w
Brain modulation after exergaming training in advanced forms of Parkinson's disease: a randomized controlled study
Abstract
Background: Physical activity combined with virtual reality and exergaming has emerged as a new technique to improve engagement and provide clinical benefit for gait and balance disorders in people with Parkinson's disease (PD).
Objective: To investigate the effects of a training protocol using a home-based exergaming system on brain volume and resting-state functional connectivity (rs-FC) in persons with PD.
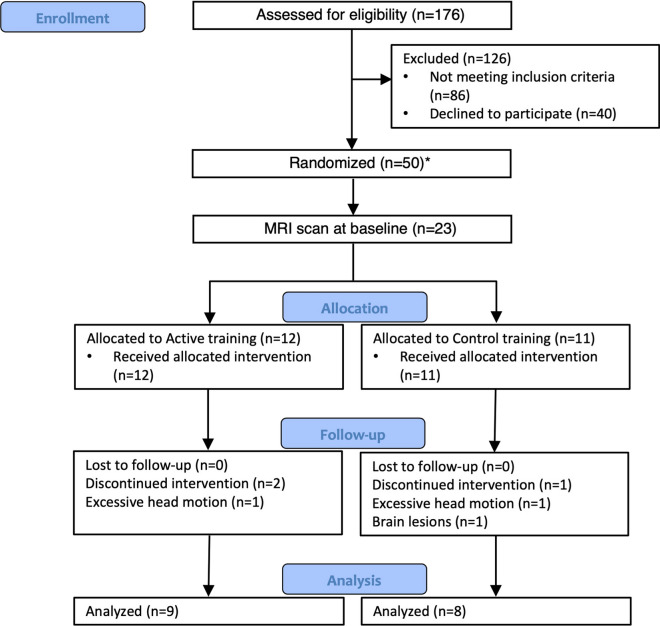
Methods: A single blind randomized controlled trial was conducted in people with PD with gait and/or balance disorders. The experimental (active) group performed 18 training sessions at home by playing a custom-designed exergame with full body movements, standing in front of a RGB-D Kinect® motion sensor, while the control group played using the computer keyboard. Both groups received the same training program. Clinical scales, gait recordings, and brain MRI were performed before and after training. We assessed the effects of both training on both the grey matter volumes (GVM) and rs-FC, within and between groups.
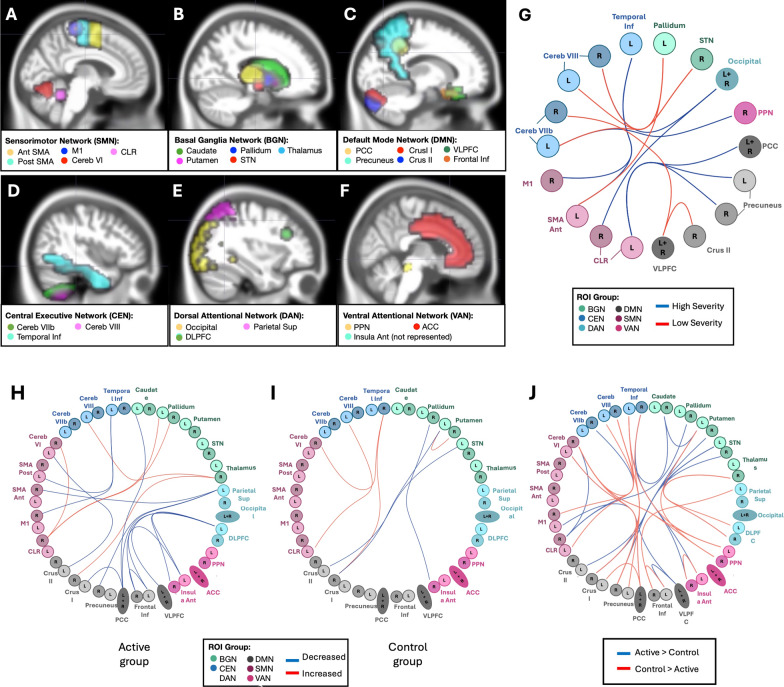
Results: Twenty-three patients were enrolled and randomly assigned to either the active (n = 11) or control (n = 12) training groups. Comparing pre- to post-training, the active group showed significant improvements in gait and balance disorders, with decreased rs-FC between the sensorimotor, attentional and basal ganglia networks, but with an increase between the cerebellar and basal ganglia networks. In contrast, the control group showed no significant changes, and rs-FC significantly decreased in the mesolimbic and visuospatial cerebellar and basal ganglia networks. Post-training, the rs-FC was greater in the active relative to the control group between the basal ganglia, motor cortical and cerebellar areas, and bilaterally between the insula and the inferior temporal lobe. Conversely, rs FC was lower in the active relative to the control group between the pedunculopontine nucleus and cerebellar areas, between the temporal inferior lobes and the right thalamus, between the left putamen and dorsolateral prefrontal cortex, and within the default mode network.
Conclusions: Full-body movement training using a customized exergame induced brain rs-FC changes within the sensorimotor, attentional and cerebellar networks in people with PD. Further research is needed to comprehensively understand the neurophysiological effects of such training approaches. Trial registration ClinicalTrials.gov NCT03560089.
Keywords: Brain magnetic resonance imaging; Exergaming; Gait disorders; Parkinson’s disease; Resting-state functional connectivity.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
